Section B:
Managing Concussion Symptoms
Introduction
 Domain 6: Headache
Domain 6: Headache
Introduction:
For patients with post-concussion headaches 1-2 weeks following acute injury, a repeat medical assessment must be conducted including a clinical history, physical examination, and the evidence-informed use of diagnostic imaging. The assessment should also include proper classification or characterization of the patient’s headache. This assessment will help identify co-morbid medical disorders (e.g., a history of migraine or non-specific headaches or psychiatric disorders) and other factors (e.g., overuse of analgesics) that can contribute to prolonged headaches. Some prolonged post-concussion headaches can be classified according to the International Classification of Headache Disorders (ICHD-III), while others cannot. Proper characterization of prolonged post-concussion headaches can help provide information to execute appropriate interdisciplinary referrals and guide evidence-based management.
Tool 6.1:Post-Concussion Headache Algorithm.
Recommendations
LEVEL OF EVIDENCE  A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)
A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study) B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)
B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations) C = Consensus, usual practice, opinion or weaker-level evidence
C = Consensus, usual practice, opinion or weaker-level evidence
6.1
Perform a repeat medical assessment on all patients presenting with post-concussion headaches 1-2 weeks following acute injury.
Include a focused history, physical examination, and consideration of diagnostic brain or cervical spine MRI imaging for those with focal or worrisome symptoms.
Tool 6.1: Post-Concussion headache algorithm.
6.1a
Take a focused clinical history.
Level of Evidence: ![]()
Collect details that help to classify or characterize the headache subtype(s) that are present.
- Headache onset, location, quality or character, severity, and frequency.
- Factors that elicit or worsen headaches (e.g., bright lights, reading, exercise, foods, etc.).
- Factors that alleviate headaches.
- Associated symptoms (e.g., aura, photosensitivity, dizziness, eye strain, neck pain).
- The presence of red flags which may indicate a more severe brain injury or other intracranial pathology (e.g., worsening headaches, repeated vomiting, weakness or numbness of the extremities, visual changes).
- The level of disability associated with the headache (e.g., missed days from school).
- Use of medications or other substances.
- Psychological or social factors or conditions that can be associated with stress and headaches (e.g., mood or anxiety disorders) (Domain 8: Mental Health).
- Assess how much headaches affect day-to-day activities.
- Disturbed sleep.
- Personal and family history of headaches and headache disorders (e.g., migraine).
- Future participation in full-contact sport or high-risk activities.
6.1b
Perform a focused physical examination.
Level of Evidence: ![]()
- Vital signs (resting heart rate and blood pressure).
- A complete neurological examination (cranial nerve, motor, sensory, reflex, cerebellar, gait and balance testing) Tool 2.1: Physical Examination.
- A cervical spine examination (palpation, range of motion, provocative cervical spine tests). Tool 2.1: Physical Examination.
- With appropriate experience, consider performing an examination of vision, oculomotor and vestibular functioning (Domain 10: Vision, Vestibular, and Oculomotor Function).
6.1c
Consider diagnostic brain or cervical spine MRI imaging for those with focal or worrisome symptoms.
Level of Evidence: ![]() CT.
CT. ![]() MRI.
MRI.
See Recommendation 2.1c for more information on when to consider diagnostic brain or cervical spine imaging.
6.1d
Classify and characterize the headache subtype based on the clinical history and physical examination findings.
Level of Evidence: ![]()
Tool 6.1: Post-Concussion Headache Algorithm.
Link: International Classification of Headache Disorders (ICHD-III)*.
Common prolonged post-concussion headache subtypes include:
- Migraine, tension, or cluster headaches.
- Cervicogenic headaches.
- Physiological or exercise-induced headaches.
- Headaches associated with prolonged visual stimulation.
- Occipital neuralgia.
* “Reproduced with permission of International Headache Society”.
6.2
Provide general post-concussion education and guidance on headache management.
6.2a
Advise on non-pharmacological strategies to minimize headaches including sleep hygiene, activity modifications, limiting triggers, and information on screen time.
Level of Evidence: ![]()
- Tool 2.7: Strategies to Promote Good Sleep and Alertness.
- Link: Sleep for Youth. CHEO Sleep Hygiene handout
- Recommendation 2.4c: Advise on the use of computers, phones, and other screen devices.
6.2b
Encourage patients with headaches to engage in cognitive activity and low-risk physical activity as soon as tolerated while staying below their symptom-exacerbation threshold. Activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) should be resumed even if mild residual symptoms are present or whenever acute symptoms improve sufficiently to permit activity.
Level of Evidence: ![]() Physical activity.
Physical activity. ![]() Cognitive activity.
Cognitive activity.
See Recommendation 2.3.
See Tool 2.6: Post-Concussion Information Sheet for examples of low-risk activities.
6.2c
Consider suggesting the use of a headache and medication diary in order to monitor symptoms and medications taken. Use clinical judgment and an individualized approach on use or duration of this strategy.
Level of Evidence: ![]()
Link: Headache and Medication Diary (Boston Children’s Hospital)
6.2d
Over-the-counter medications such as acetaminophen and ibuprofen may be recommended to treat acute headache. Advise on limiting the use of these medications to less than 15 days a month and avoiding “around-the-clock” dosing to prevent overuse or rebound headaches. I.e., advise that children/adolescents avoid using over the counter medications at regular scheduled times throughout the day.
Level of Evidence: ![]()
6.3
Refer patients who have prolonged post-concussion headaches for more than 4 weeks to an interdisciplinary concussion team or to a sub-specialist for further evaluation and management. Consider early referral (prior to 4-weeks after the acute injury) to an interdisciplinary concussion team in the presence of modifiers that may delay recovery.
Level of Evidence: ![]()
Prolonged headaches in pediatric concussion patients can be difficult to classify and manage and can co-occur with other prolonged post-concussion symptoms (dizziness, neck pain, sleep disturbance, cognitive or mood challenges).
If an interdisciplinary concussion team member is not available:
- Consider appropriate referral to interdisciplinary professionals who have competency-based training and clinical experience to independently manage the identified headaches and headache disorders.
If a child/adolescent with prolonged post-concussion headache has not had a recent vision assessment, refer to an optometrist for an assessment.
6.4
Consider initiating pharmacological therapy to treat and manage prolonged headaches while waiting for the interdisciplinary concussion team or sub-specialist referral.
Level of Evidence: ![]()
For patients with post-traumatic headaches that are migrainous in nature, the use of migraine-specific abortants such as triptan class medications may be used if effective. Due to the risk of developing medication-induced headaches, limit use of abortants to fewer than 6-10 days per month.
Tool 6.2: General Considerations Regarding Pharmacotherapy.
Tool 6.3: Approved Medications for Pediatric Indications.
Prophylactic therapy should be considered:
- If headaches are occurring frequently.
- If headaches are disabling.
- If acute headache medications are contraindicated or poorly tolerated or are being used too frequently.
6.5
Recommend a medical follow-up to reassess clinical status if headaches persist. Recommend an immediate medical follow-up in the presence of any deterioration. Consider early referral (prior to 4-weeks after the acute injury) to an interdisciplinary concussion team in the presence of modifiers that may delay recovery.
Level of Evidence: ![]() Medical follow-up.
Medical follow-up. ![]() Early referral in the presence of modifiers that may delay recovery.
Early referral in the presence of modifiers that may delay recovery.
Specialized interdisciplinary concussion care is ideally initiated for patients at elevated risk for a delayed recovery within the first two weeks post-injury.
Level of Evidence: B
See Recommendation 2.2: Note any modifiers that may delay recovery and use a clinical risk score to predict risk of prolonged symptoms.
Tools and Resources
Living Guideline Tools:
- Tool 2.1: Physical Examination
- Tool 6.1: Post-Concussion Headache Algorithm
- Tool 2.6 Post-Concussion Information Sheet (Updated Sept 2023)
- Tool 2.7: Strategies to Promote Good Sleep and Alertness
- Tool 6.2: General Considerations Regarding Pharmacotherapy
- Tool 6.3: Approved Medications for Pediatric Indications
Online Tools to Consider:
References
Click here to access the Living Guideline Evidence Map (powered by EPPIreviewer and EPPIvisualizer)
Reference List: Last updated Sept 2023, update in progress (April 2024).
Ali Muhammad, Asghar Nek, Hannah Theodore, Schupper Alexander J, Li Adam, Dreher Nickolas, Murtaza-Ali Muhammad, Vasan Vikram, Nakadar Zaid, Alasadi Husni, Lin Anthony, Hrabarchuk Eugene, Quinones Addison, McCarthy Lily, Asfaw Zerubabbel, Dullea Jonathan, Gometz Alex, Lovell Mark, and Choudhri Tanvir (2023) A multicenter, longitudinal survey of headaches and concussions among youth athletes in the United States from 2009 to 2019. The Journal of Headache and Pain 24(1), 6
Bramley Harry, Heverley Steven, Lewis Mechelle M, Kong Lan, Rivera Rowena, and Silvis Matthew (2015) Demographics and Treatment of Adolescent Posttraumatic Headache in a Regional Concussion Clinic. Pediatric Neurology 52(5), 493-498 DOI: 10.1016/j.pediatrneurol.2015.01.008
Bresee Natalie, Aglipay Mary, Dubrovsky Alexander Sasha, Ledoux Andrée-anne Anne, Momoli Franco, Gravel Jocelyn, Freedman Stephen B, Barlow Karen, Richer Lawrence, Barrowman Nicholas J, and Zemek Roger (2018) No association between metoclopramide treatment in ED and reduced risk of post-concussion headache. American Journal of Emergency Medicine 36(12), 2225-2231 DOI: 10.1016/j.ajem.2018.04.007
Cushman Daniel M, Borowski Lauren, Hansen Colby, Hendrick John, Bushman Troy, and Teramoto Masaru (2019) Gabapentin and Tricyclics in the Treatment of Post-Concussive Headache, a Retrospective Cohort Study. Headache 59(3), 371-382 DOI: 10.1111/head.13451
Eckner James T, Seifert Tad, Pescovitz Allison, Zeiger Max, and Kutcher Jeffrey S (2017) Is migraine headache associated with concussion in athletes? A case-control study. Clinical Journal of Sport Medicine 27(3), 266-270 DOI: 10.1097/JSM.0000000000000346
Ellis Michael J, Cordingley Dean, Girardin Richard, Ritchie Lesley, and Johnston Janine (2017) Migraine with aura or sports-related concussion: Case report, pathophysiology, and multidisciplinary approach to management. Current Sports Medicine Reports 16(1), 14-18 DOI: 10.1249/JSR.0000000000000323
Heyer Geoffrey L, Young Julie A, Rose Sean C, McNally Kelly A, and Fischer Anastasia N (2015) Post-traumatic headaches correlate with migraine symptoms in youth with concussion. Cephalalgia 36(4), 309-316 DOI: 10.1177/0333102415590240
Kamins Joshua, Richards Rachel, Barney Bradley J, Locandro Christopher, Pacchia Christina F, Charles Andrew C, Cook Lawrence J, Gioia Gerard, Giza Christopher C, and Blume Heidi K (2021) Evaluation of Posttraumatic Headache Phenotype and Recovery Time After Youth Concussion. JAMA network open 4(3), e211312
Klein Susan K, Brown Cynthia B, Ostrowski-Delahanty Sarah, Bruckman David, and Victorio M Cristina (2022) Identifying Migraine Phenotype Post Traumatic Headache (MPTH) to Guide Overall Recovery From Traumatic Brain Injury. Journal of Child Neurology , 8830738221100327
Kontos Anthony P, Elbin R J, Lau Brian, Simensky Steven, Freund Brin, French Jonathan, and Collins Michael W (2013) Posttraumatic migraine as a predictor of recovery and cognitive impairment after sport-related concussion. American Journal of Sports Medicine 41(7), 1497-1504 DOI: 10.1177/0363546513488751
Kuczynski Andrea, Crawford Susan, Bodell Lisa, Dewey Deborah, and Barlow Karen M (2013) Characteristics of post-traumatic headaches in children following mild traumatic brain injury and their response to treatment: A prospective cohort. Developmental Medicine and Child Neurology 55(7), 636-641 DOI: 10.1111/dmcn.12152
Kwan Vivian, Plourde Vickie, Yeates Keith Owen, Noel Melanie, and Brooks Brian L (2020) Headache long after pediatric concussion: presence, intensity, interference, and association with cognition. Brain Injury 34(4), 575-582 DOI: 10.1080/02699052.2020.1725842
Lambrinakos-Raymond Kristen, Dubrovsky Alexander Sasha, Gagnon Isabelle, Zemek Roger, and Burstein Brett (2021) Management of Pediatric Post-Concussion Headaches: National Survey of Abortive Therapies Used in the Emergency Department. Journal of Neurotrauma ,
Ledoux Andree, Tang Ken, Freedman Stephen B, Gravel Jocelyn, Boutis Kathy, Yeates Keith O, Mannix Rebekah C, Richer Lawrence R, Bell Michael J, Zemek Roger L, Pediatric Emergency, and Research Canada (2022) Early analgesic administration and headache presence 7 days post-concussion in children. CJEM ,
Marbil Mica Gabrielle, Ware Ashley L, Galarneau Jean Michel, Minich Nori Mercuri, Hershey Andrew D, Orr Serena L, Defta Dana M, Taylor H Gerry, Bigler Erin D, Cohen Daniel M, Mihalov Leslie K, Bacevice Ann, Bangert Barbara A, and Yeates Keith Owen (2023) Longitudinal trajectories of posttraumatic headache after pediatric mild traumatic brain injury. Cephalalgia : an international journal of headache 43(5), 3331024231161740
McCarthy Lily, Hannah Theodore C, Li Adam Y, Schupper Alexander J, Hrabarchuk Eugene, Kalagara Roshini, Ali Muhammad, Gometz Alex, Lovell Mark R, and Choudhri Tanvir F (2022) Effects of a history of headache and migraine treatment on baseline neurocognitive function in young athletes. The Journal of Headache and Pain 23(1), 62
McEvoy Haley, Borsook David, and Holmes Scott A (2020) Clinical features and sex differences in pediatric post-traumatic headache: A retrospective chart review at a Boston area concussion clinic. Cephalalgia 40(7), 701-711 DOI: 10.1177/0333102419896754
Mihalik Jason P, Register-Mihalik Johna, Kerr Zachary Y, Marshall Stephen W, McCrea Michael C, and Guskiewicz Kevin M (2013) Recovery of posttraumatic migraine characteristics in patients after mild traumatic brain injury. American Journal of Sports Medicine 41(7), 1490-1496 DOI: 10.1177/0363546513487982
Murray Thomas R, Ferderer Tanner, Gehred Alison, and Rose Sean C (2021) Treatment of Post-traumatic Headaches in Children: A Systematic Review. Seminars in Pediatric Neurology 40, 100935
Pasek Tracy Annz, Locasto Lisa W, Reichard Joseph, Fazio Sumrok, Vanessa C, Johnson Eric W, and Kontos Anthony P (2015) The headache electronic diary for children with concussion. Clinical Nurse Specialist 29(2), 80-88 DOI: 10.1097/NUR.0000000000000108
Patterson Gentile Carlyn, Shah Ryan, Irwin Samantha L, Greene Kaitlin, and Szperka Christina L (2021) Acute and chronic management of posttraumatic headache in children: A systematic review. Headache 61(10), 1475-1492
Seeger Trevor A, Orr Serena, Bodell Lisa, Lockyer Lisette, Rajapakse Thilinie, and Barlow Karen M (2015) Occipital nerve blocks for pediatric posttraumatic headache: A case series. Journal of Child Neurology 30(9), 1142-1146 DOI: 10.1177/0883073814553973
Shaw Lauren, Morozova Maria, and Abu-Arafeh Ishaq (2018) Chronic post-traumatic headache in children and adolescents: systematic review of prevalence and headache features. Pain management 8(1), 57-64 DOI: 10.2217/pmt-2017-0019
Sufrinko Alicia, McAllister-Deitrick Jamie, Elbin Rj, Collins Michael W, and Kontos Anthony P (2018) Family History of Migraine Associated with Posttraumatic Migraine Symptoms Following Sport-Related Concussion. Journal of Head Trauma Rehabilitation 33(1), 7-14 DOI: 10.1097/HTR.0000000000000315
Sussman Walter I, Mautner Ken, Mason R Amadeus, Bonecutter Kathryn, and Shealy Anna K (2017) Sphenopalatine ganglion block for management of refractory chronic posttraumatic headaches after a sport-related concussion. Clinical Journal of Sport Medicine 27(2), e6-e8 DOI: 10.1097/JSM.0000000000000325
Terry Douglas P, Reddi Preethi J, Cook Nathan E, Seifert Tad, Maxwell Bruce A, Zafonte Ross, Berkner Paul D, and Iverson Grant L (2019) Acute Effects of Concussion in Youth With Pre-existing Migraines. Clinical Journal of Sport Medicine Publish Ahead of Print(00), DOI: 10.1097/jsm.0000000000000791
van Ierssel Jacqueline Josee, Tang Ken, Beauchamp Miriam, Bresee Natalie, Cortel-LeBlanc Achelle, Craig William, Doan Quynh, Gravel Jocelyn, Lyons Todd, Mannix Rebekah, Orr Serena, Zemek Roger, and Yeates Keith Owen (2023) Association of Posttraumatic Headache With Symptom Burden After Concussion in Children. JAMA network open 6(3), e231993
Yengo-Kahn Aaron M, Hibshman Natalie, Bonfield Christopher M, Torstenson Eric S, Gifford Katherine A, Belikau Daniil, Davis Lea K, Zuckerman Scott L, and Dennis Jessica K (2022) Association of Preinjury Medical Diagnoses With Pediatric Persistent Postconcussion Symptoms in Electronic Health Records. The Journal of head trauma rehabilitation 37(2), E80-E89
 Domain 7: Sleep
Domain 7: Sleep
Introduction:
Information related to sleep hygiene and non-pharmacological strategies to improve sleep should be shared with families. Children/adolescents with prolonged sleep disturbances should be encouraged to engage in low-risk physical activity and resume sub-symptom cognitive activities. Children/adolescents who are experiencing sleep disturbances more than 4 weeks following a concussion should be referred to a cognitive behavioural therapist or an interdisciplinary concussion team. If sleep disturbances are present for more than 6 weeks following a concussion the child/adolescent may require more specialized care from a sleep specialist.
Tool 7.1: Managing post-concussion sleep disturbances algorithm.
Tool 7.2: Factors that may influence the child/adolescent’s sleep/wake cycle.
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
7.1
Perform a repeat medical assessment on all patients presenting with post-concussion sleep disturbances 1-2 weeks following acute injury.
Level of Evidence: ![]()
Include a focused history, physical examination, and consider diagnostic brain or cervical spine MRI imaging for those with focal or worrisome symptoms.
Screen for factors that may influence the child/adolescent’s sleep/wake cycle and for sleep-wake disturbances such as insomnia or excessive daytime sleepiness.
7.2
Provide general education and guidance on sleep hygiene that outlines non-pharmacological strategies to improve sleep.
Level of Evidence: ![]()
7.2a
Continue to encourage patients with sleep disturbances to engage in sub-symptom threshold cognitive activities and physical activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) as soon as tolerated.
Level of Evidence: ![]() Gradual return to physical activity.
Gradual return to physical activity. ![]() Gradual return to cognitive activity.
Gradual return to cognitive activity.
See Recommendation 2.3.
See Tool 2.6: Post-Concussion Information Sheet for examples of low-risk activities.
7.3
Consider managing patients who experience sleep-wake disturbances for more than 4 weeks with cognitive behavioural therapy, treat with daily supplements, and/or refer to an interdisciplinary concussion team.
Level of Evidence: ![]()
7.3a
Refer the child/adolescent to a cognitive behavioural specialist. The treatment of choice for primary insomnia and insomnia co-morbid to a medical or psychiatric condition is cognitive behavioural therapy (CBT).
Level of Evidence: ![]()
If CBT is unavailable to the patient or the patient is waiting for CBT treatment:
- Optimize and implement sleep hygiene (Tool 2.7: Strategies to Promote Good Sleep and Alertness)
- Monitor the patient weekly for the first few weeks.
- Re-emphasize that patients with sleep disturbances should continue to engage in sub-symptom threshold cognitive and physical activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) as tolerated (Recommendation 2.3).
- Consider referring to an interdisciplinary concussion team.
7.3b
Consider suggesting non-pharmacological supplements such as magnesium, melatonin*, and zinc to improve sleep and recovery without the use of medication that may have side effects.
Level of Evidence: ![]()
*Melatonin was not found to be effective when used for youth with concussion symptoms 4-6 weeks after injury in a single-center double-blinded randomized controlled trial” (Barlow et al 2020. Efficacy of Melatonin in Children With Postconcussive Symptoms: A Randomized Clinical Trial. Pediatrics
7.4
Refer patients with prolonged post-concussion sleep disturbances (more than 6 weeks) to a sleep specialist or an interdisciplinary concussion team if the interventions introduced at 4 weeks have been unsuccessful and sleep issues persist.
Level of Evidence: ![]()
If sleep issues persist for more than 6 weeks post-acute injury, sleep hygiene can’t be optimized, and if poor sleep quality is impacting the ability to return-to-school or ability to recondition:
- Refer to a sleep specialist who has experience with concussion and polysomnography or to an interdisciplinary concussion team that has the expertise to understand sleep disturbances in the context of concussion-related symptoms.
Consider ordering sleep tests to rule out possible sleep-related breathing disorders, nocturnal seizures, periodic limb movements, or narcolepsy.
- Examples of sleep tests include Sleep Study, Multiple Sleep Latency Test, and the Maintenance of Wakefulness Test.
7.5
Consider prescribing medication on a short-term basis if sleep has not improved after 6 weeks following the acute injury.
Level of Evidence: ![]()
Ensure that medications do not result in dependency and that the patient has minimal adverse effects. The aim is to establish a more routine sleep pattern.
- Potential medication options include trazodone 12.5 mg or amitriptyline 5.0 – 10.0 mg.
- Tool 6.2: General Considerations Regarding Pharmacotherapy.
- Tool 6.3: Approved Medications for Pediatric Indications.
If sleep disturbances persist after pharmacological treatment refer to a pediatric sleep specialist ideally with experience with concussion and polysomnography.
7.6
Recommend a medical follow-up to reassess clinical status if sleep disturbances persist. Recommend an immediate medical follow-up in the presence of any deterioration. Consider early referral (before 4 weeks) to an interdisciplinary concussion team in the presence of modifiers that may delay recovery.
Level of Evidence: ![]() Medical follow-up.
Medical follow-up. ![]() Early referral in the presence of modifiers that may delay recovery.
Early referral in the presence of modifiers that may delay recovery.
Specialized interdisciplinary concussion care is ideally initiated for patients at elevated risk for a delayed recovery within the first two weeks post-injury.
Level of Evidence: B
See Recommendation 2.1b: Note any modifiers that may delay recovery and use a clinical risk score to predict risk of prolonged symptoms.
Tools and Resources
Living Guideline Tools:
- Tool 2.6: Post-Concussion Information Sheet
- Tool 2.7: Strategies to Promote Good Sleep and Alertness
- Tool 6.2: General Considerations Regarding Pharmacotherapy
- Tool 6.3: Approved Medications for Pediatric Indications
- Tool 7.1: Managing Post-Concussion Sleep Disturbances Algorithm
- Tool 7.2: Factors that may influence the child/adolescent’s sleep/wake cycle
Online Tools to Consider:
- Concussion & You Handbook (Holland Bloorview Kids Rehabilitation Hospital)
- Sleep for Youth. CHEO Sleep Hygiene handout
References
Research papers that support the present guideline recommendations:
Beebe, D. W., Powers, S. W., Slattery, E. W., & Gubanich, P. J. (2017). Short Sleep and Adolescentsʼ Performance on a Concussion Assessment Battery: An Experimental Sleep Manipulation Study. Clinical Journal of Sport Medicine, 0(0), 1. https://doi.org/10.1097/JSM.0000000000000454
Blake, M., Schwartz, O., Waloszek, J.M., Raniti, M., Simmons, J.G., … Allen, N.B. (2017). The SENSE Study: Treatment Mechanisms of a Cognitive Behavioral and Mindfulness-Based Group Sleep Improvement Intervention for At-Risk Adolescents. Sleep. 40(6). https://doi.org/10.1093/sleep/zsx061
Botchway, E. N., Godfrey, C., Anderson, V., & Catroppa, C. (2019). A Systematic Review of Sleep-Wake Disturbances in Childhood Traumatic Brain Injury: Relationship with Fatigue, Depression, and Quality of Life. The Journal of Head Trauma Rehabilitation, 34(4), 241–256. https://doi.org/10.1097/HTR.0000000000000446
Bramley, H., Henson, A., Lewis, M. M., Kong, L., Stetter, C., & Silvis, M. (2017). Sleep Disturbance Following Concussion Is a Risk Factor for a Prolonged Recovery. Clinical Pediatrics, 56(14), 1280–1285. https://doi.org/10.1177/0009922816681603
Brooks, B. L., Sayers, P. Q., Virani, S., Rajaram, A. A., & Tomfohr-Madsen, L. (2019). Insomnia in adolescents with slow recovery from concussion. Journal of Neurotrauma, 36(16), 2391–2399. https://doi.org/10.1089/neu.2018.6257
Crichton, A., Oakley, E., Babl, F. E., Greenham, M., Hearps, S., Delzoppo, C., … Anderson, V. (2018). Predicting Fatigue 12 Months after Child Traumatic Brain Injury: Child Factors and Postinjury Symptoms. Journal of the International Neuropsychological Society, 24(3), 224–236. https://doi.org/10.1017/S1355617717000893
de Bruin, E.J., Bögels, S.M., Oort, F.J., Meijer, A.M. (2015). Efficacy of Cognitive Behavioral Therapy for Insomnia in Adolescents: A Randomized Controlled Trial with Internet Therapy, Group Therapy and A Waiting List Condition. Sleep. 38(12),1913-1926. https://doi.org/10.5665/sleep.5240
Gradisar, M., Dohn, H., Gardner, G., Paine, S., Starkey, K … Trenowden, S. (2011). A Randomized Controlled Trial of Cognitive-Behavior Therapy Plus Bright Light Therapy for Adolescent Delayed Sleep Phase Disorder. Sleep. 34(12),1671-1680. https://doi.org/10.5665/sleep.1432
Howell, D. R., Oldham, J. R., Brilliant, A. N., & Meehan, W. P. (2019). Trouble Falling Asleep After Concussion Is Associated With Higher Symptom Burden Among Children and Adolescents. Journal of Child Neurology, 34(5), 256–261. https://doi.org/10.1177/0883073818824000
Kostyun, R. O., Milewski, M. D., & Hafeez, I. (2015). Sleep disturbance and neurocognitive function during the recovery from a sport-related concussion in adolescents. American Journal of Sports Medicine, 43(3), 633–640. https://doi.org/10.1177/0363546514560727
Landry-Roy, C., Bernier, A., Gravel, J., & Beauchamp, M. H. (2018). Executive Functions and Their Relation to Sleep Following Mild Traumatic Brain Injury in Preschoolers. Journal of the International Neuropsychological Society, 24(8), 769–780. https://doi.org/10.1017/S1355617718000401
Lin, K., & Tung, C. (2016). Acupuncture for Recovery from Pediatric Sport-Related Concussion. Medical Acupuncture, 28(4), 217–222. https://doi.org/10.1089/acu.2016.1181
Meng, X., Li, Y., Li, S., Zhou, Y., Gan, R. Y., Xu, D. P., & Li, H. B. (2017). Dietary Sources and Bioactivities of Melatonin. Nutrients, 9(4), 367. https://doi.org/10.3390/nu9040367
Murdaugh, D. L., Ono, K. E., Reisner, A., & Burns, T. G. (2018). Assessment of Sleep Quantity and Sleep Disturbances During Recovery From Sports-Related Concussion in Youth Athletes. Archives of Physical Medicine and Rehabilitation, 99(5), 960–966. https://doi.org/10.1016/j.apmr.2018.01.005
Schmidt, A. T., Li, X., Hanten, G. R., McCauley, S. R., Faber, J., & Levin, H. S. (2015). A longitudinal investigation of sleep quality in adolescents and young adults after mild traumatic brain injury. Cognitive and Behavioral Neurology, 28(2), 53–62. https://doi.org/10.1097/WNN.0000000000000056
Sunnybrook Health Science Centre. Sleep Issues After Concussion. https://sunnybrook.ca/content/?page=bsp-concussion-sleep-tips
Tham, S. W., Fales, J., & Palermo, T. M. (2015). Subjective and Objective Assessment of Sleep in Adolescents with Mild Traumatic Brain Injury. Journal of Neurotrauma, 32(11), 847–852. https://doi.org/10.1089/neu.2014.3559
Theadom, A., Starkey, N., Jones, K., Cropley, M., Parmar, P., Barker-Collo, S., & Feigin, V. L. (2016). Sleep difficulties and their impact on recovery following mild traumatic brain injury in children. Brain Injury, 30(10), 1243–1248. https://doi.org/10.1080/02699052.2016.1183171
Wiseman-Hakes, C., Gosselin, N., Sharma, B., Langer, L., & Gagnon, I. (2019). A Longitudinal Investigation of Sleep and Daytime Wakefulness in Children and Youth With Concussion. ASN Neuro, 11. https://doi.org/10.1177/1759091418822405
Research papers not associated with a current recommendation:
van Markus-Doornbosch, F., Peeters, E., van der Pas, S., Vlieland, T. V., & Meesters, J. (2019). Physical activity after mild traumatic brain injury: What are the relationships with fatigue and sleep quality? European Journal of Paediatric Neurology, 23(1), 53–60. https://doi.org/10.1016/j.ejpn.2018.11.002
Last update: November 16, 2019
 Domain 8: Mental Health and Psychosocial Factors
Domain 8: Mental Health and Psychosocial Factors
Introduction:
Early identification of family problems or parental mental health disorders permits healthcare professionals to watch for environmental factors that are known to influence recovery from a concussion and identify any associated negative outcomes.
It is important to:
- Assess if there is an association between concussion symptoms and restrictions to activity that may be related to the child/adolescent’s mental health.
- Treat and manage the mental health disorder itself and prevent it from becoming a long-term problem.
- Encourage the child/adolescent to remain connected and engage with their peers, friends, and teammates.
Tool 8.1: Post-Concussion Mental Health Considerations Algorithm.
Tool 8.2: Management of Prolonged Mental Health Disorders Algorithm.
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
8.1
Assess existing and new mental health symptoms and disorders.
Level of Evidence: ![]()
Experienced and trained healthcare professionals should use appropriate screening tools to assess the child/adolescent. These assessments should be considered for children/adolescents with a history of mental health problems or with prolonged post-concussive symptoms.
Use Tool 8.1: Post-concussion mental health considerations algorithm and refer to a mental health specialist using clinical judgment.
Assessment screening tools to consider (direct website links):
- Link: PHQ-SADS (somatic)
- Link: Severity Measure for Depression- Child Age 11–17 (adapted from PHQ-9 modified for Adolescents [PHQ-A])
- Link: Severity Measure for Generalized Anxiety Disorder-Child Age 11–17 (adapted from GAD-7)
- Link: HEADS-ED Tool—Screening for Pediatric Mental Health (online interactive tool)
- Link: PROMIS Anxiety (pediatric and parent versions are available via HealthMeasures.net)
- Link: PROMIS Depression (pediatric and parent versions are available via HealthMeasures.net)
- Link: PROMIS Profile (25 questions, 37 questions, 49 questions versions are available via HealthMeasures.net)
8.2
Assess the child/adolescent’s broader environment, including family and caregiver function, mental health, and social connections.
Level of Evidence: ![]()
- Ask about socioeconomic status (caregiver education, family income, occupation).
- Ask about social impacts and life stressors (school setting, friends, teammates).
- Ask the child/adolescent and parents and/or caregivers to complete the following, as appropriate:
- Link: PROMIS Family Function (pediatric and parent versions are available via HealthMeasures.net)
- Link: Patient Health Questionnaire (PHQ-9) (Self-administered screen for depression in adults)
- Link: Generalized Anxiety Disorder scale (GAD-7)
8.3
Treat mental health symptoms or refer to a specialist in pediatric mental health.
Level of Evidence: ![]()
Base the mental health treatment on individual factors, patient preferences, the severity of symptoms, and co-morbidities.
Tools to assist healthcare professionals to make treatment decisions:
- Tool 8.1: Post-Concussion Mental Health Considerations Algorithm.
- Tool 8.2: Management of Prolonged Mental Health Disorders Algorithm.
- Tool 6.2: General Considerations Regarding Pharmacotherapy.
- Tool 6.3: Approved Medications for Pediatric Indications.
Consider referring to a local healthcare professional, specialized pediatric concussion program or to a specialist with experience in pediatric mental health if child/adolescent has prolonged or urgent mental health symptoms. Provide the name of a specialist with experience in pediatric mental health.
For deciding when to refer a child/adolescent to a specialist, use Tool 8.1: Post-Concussion Mental Health Considerations Algorithm.
Tools and Resources
Living Guideline Tools:
- Tool 6.2: General Considerations Regarding Pharmacotherapy
- Tool 6.3: Approved Medications for Pediatric Indications.
- Tool 8.1: Post-Concussion Mental Health Considerations Algorithm
- Tool 8.2: Management of Prolonged Mental Health Disorders Algorithm
Assessment screening tools to consider (website links):
- Generalized Anxiety Disorder scale (GAD-7)
- HEADS-ED Tool—Screening for Pediatric Mental Health (online interactive tool)
- Patient Health Questionnaire (PHQ-9) (A self-administered screen for depression in adults)
- PHQ-SADS (somatic)
- PROMIS Anxiety (pediatric and parent versions are available via HealthMeasures.net)
- PROMIS Depression (pediatric and parent versions are available via HealthMeasures.net)
- PROMIS Profile (25 questions, 37 questions, 49 questions versions are available via HealthMeasures.net)
- PROMIS Family Function (pediatric and parent versions are available via HealthMeasures.net)
- Severity Measure for Depression- Child Age 11–17 (adapted from PHQ-9 modified for Adolescents [PHQ-A])
- Severity Measure for Generalized Anxiety Disorder-Child Age 11–17 (adapted from GAD-7)
References
Research papers that support the present guideline recommendations:
Babikian, T., McArthur, D., & Asarnow, R. F. (2013). Predictors of 1-month and 1-year neurocognitive functioning from the UCLA longitudinal mild, uncomplicated, pediatric traumatic brain injury study. Journal of the International Neuropsychological Society, 19(2), 145–154. https://doi.org/10.1017/S135561771200104X
Bellerose, J., Bernier, A., Beaudoin, C., Gravel, J., & Beauchamp, M. H. (2017). Long-term brain-injury-specific effects following preschool mild TBI: A study of theory of mind. Neuropsychology, 31(3), 229–241. https://doi.org/10.1037/neu0000341
Bernard, C. O., Ponsford, J. A., McKinlay, A., McKenzie, D., & Krieser, D. (2016). Predictors of post-concussive symptoms in young children: Injury versus non-injury related factors. Journal of the International Neuropsychological Society, 22(8), 793–803. https://doi.org/10.1017/S1355617716000709
Biederman, J., Feinberg, L., Chan, J., Adeyemo, B. O., Woodworth, K. Y., Panis, W., … Faraone, S. V. (2015). Mild traumatic brain injury and attention-deficit hyperactivity disorder in young student athletes. Journal of Nervous and Mental Disease, 203(11), 813–819. https://doi.org/10.1097/NMD.0000000000000375
Bonfield, C. M., Lam, S., Lin, Y., & Greene, S. (2013). The impact of attention deficit hyperactivity disorder on recovery from mild traumatic brain injury. Journal of Neurosurgery: Pediatrics, 12(2), 97–102. https://doi.org/10.3171/2013.5.PEDS12424
Brooks, B. L., Plourde, V., Beauchamp, M. H., Tang, K., Yeates, K. O., Keightley, M., … Zemek, R. (2019). Predicting Psychological Distress after Pediatric Concussion. Journal of Neurotrauma, 36(5), 679–685. https://doi.org/10.1089/neu.2018.5792
Chasle, V., Riffaud, L., Longuet, R., Martineau-Curt, M., Collet, Y., Le Fournier, L., & Pladys, P. (2016). Mild head injury and attention deficit hyperactivity disorder in children. Child’s Nervous System, 32(12), 2357–2361. https://doi.org/10.1007/s00381-016-3230-z
Chrisman, S. P. D., & Richardson, L. P. (2014). Prevalence of diagnosed depression in adolescents with history of concussion. Journal of Adolescent Health, 54(5), 582–586. https://doi.org/10.1016/j.jadohealth.2013.10.006
Connolly, E. J., & McCormick, B. F. (2019). Mild Traumatic Brain Injury and Psychopathology in Adolescence: Evidence From the Project on Human Development in Chicago Neighborhoods. Journal of Adolescent Health, 65(1), 79–85. https://doi.org/10.1016/j.jadohealth.2018.12.023
Cook, N. E., Kelshaw, P. M., Caswell, S. V., & Iverson, G. L. (2019). Children with Attention-Deficit/Hyperactivity Disorder Perform Differently on Pediatric Concussion Assessment. Journal of Pediatrics, 214, 168-174.e1. https://doi.org/10.1016/j.jpeds.2019.07.048
Corwin, D. J., Zonfrillo, M. R., Master, C. L., Arbogast, K. B., Grady, M. F., Robinson, R. L., … Wiebe, D. J. (2014). Characteristics of Prolonged Concussion Recovery in a Pediatric Subspecialty Referral Population. The Journal of Pediatrics, 165(6), 1207–1215. https://doi.org/10.1016/j.jpeds.2014.08.034
Donders, J., & DeWit, C. (2017). Parental ratings of daily behavior and child cognitive test performance after pediatric mild traumatic brain injury. Child Neuropsychology, 23(5), 554–570. https://doi.org/10.1080/09297049.2016.1161015
Eisenberg, M. A., Meehan, W. P., & Mannix, R. (2014). Duration and Course of Post-Concussive Symptoms. Pediatrics, 133(6), 999–1006. https://doi.org/10.1542/peds.2014-0158
Elbin, R. J., Kontos, A. P., Kegel, N., Johnson, E., Burkhart, S., & Schatz, P. (2013). Individual and combined effects of LD and ADHD on computerized neurocognitive concussion test performance: Evidence for separate norms. Archives of Clinical Neuropsychology, 28(5), 476–484. https://doi.org/10.1093/arclin/act024
Ellis, M. J., Ritchie, L. J., Koltek, M., Hosain, S., Cordingley, D., Chu, S., … Russell, K. (2015). Psychiatric outcomes after pediatric sports-related concussion. Journal of Neurosurgery: Pediatrics, 16(6), 709–718. https://doi.org/10.3171/2015.5.PEDS15220
Gardner, R. M., Yengo-Kahn, A., Bonfield, C. M., & Solomon, G. S. (2017). Comparison of baseline and post-concussion ImPACT test scores in young athletes with stimulant-treated and untreated ADHD. Physician and Sportsmedicine, 45(1), 1–10. https://doi.org/10.1080/00913847.2017.1248221
Gornall, A., Takagi, M., Clarke, C., Babl, F. E., Davis, G. A., Dunne, K., … Anderson, V. (2019). Behavioral and Emotional Difficulties after Pediatric Concussion. Journal of Neurotrauma, 1–26. https://doi.org/10.1089/neu.2018.6235
Guerriero, R. M., Kuemmerle, K., Pepin, M. J., Taylor, A. M., Wolff, R., & Meehan, W. P. (2018). The Association Between Premorbid Conditions in School-Aged Children With Prolonged Concussion Recovery. Journal of Child Neurology, 33(2), 168–173. https://doi.org/10.1177/0883073817749655
Guo, X., Edmed, S. L., & Anderson, V. (2017). Neurocognitive predictors of posttraumatic stress disorder symptoms in children 6 months after traumatic brain injury: A prospective study. Neuropsychology, 31(1), 84–92. https://doi.org/http://dx.doi.org/10.1037/neu0000305
Hunt, A. W., Paniccia, M., Reed, N., & Keightley, M. (2016). Concussion-Like Symptoms in Child and Youth Athletes at Baseline: What Is “Typical”? Journal of Athletic Training, 51(10), 749–757. https://doi.org/10.4085/1062-6050-51.11.12
Jimenez, N., Quistberg, A., Vavilala, M. S., Jaffe, K. M., & Rivara, F. P. (2017). Utilization of Mental Health Services After Mild Pediatric Traumatic Brain Injury. Pediatrics, 139(3), e20162462. https://doi.org/10.1542/peds.2016-2462
Jones, K. M., Prah, P., Starkey, N., Theadom, A., Barker-Collo, S., Ameratunga, S., … Brown, P. (2019). Longitudinal patterns of behavior, cognition, and quality of life after mild traumatic brain injury in children: BIONIC study findings. Brain Injury, 33(7), 884–893. https://doi.org/10.1080/02699052.2019.1606445
Kaldoja, M.-L., & Kolk, A. (2015). Does Gender Matter? Differences in Social-Emotional Behavior Among Infants and Toddlers Before and After Mild Traumatic Brain Injury. Journal of Child Neurology, 30(7), 860–867. https://doi.org/10.1177/0883073814544705
Kirkwood, M. W., Peterson, R. L., Connery, A. K., Baker, D. A., & Forster, J. (2016). A Pilot Study Investigating Neuropsychological Consultation as an Intervention for Persistent Postconcussive Symptoms in a Pediatric Sample. Journal of Pediatrics, 169, 244–249e1. https://doi.org/10.1016/j.jpeds.2015.10.014
Liou, Y. J., Wei, H. T., Chen, M. H., Hsu, J. W., Huang, K. L., Bai, Y. M., … Chen, T. J. (2018). Risk of Traumatic Brain Injury Among Children, Adolescents, and Young Adults With Attention-Deficit Hyperactivity Disorder in Taiwan. Journal of Adolescent Health, 63(2), 233–238. https://doi.org/10.1016/j.jadohealth.2018.02.012
Mac Donald, C. L., Barber, J., Wright, J., Coppel, D., De Lacy, N., Ottinger, S., … Temkin, N. (2019). Longitudinal Clinical and Neuroimaging Evaluation of Symptomatic Concussion in 10-to 14-year-old Youth Athletes. Journal of Neurotrauma, 36(2), 264–274. https://doi.org/10.1089/neu.2018.5629
Max, J. E., Friedman, K., Wilde, E. A., Bigler, E. D., Hanten, G., Schachar, R. J., … Levin, H. S. (2015). Psychiatric disorders in children and adolescents 24 months after mild traumatic brain injury. Journal of Neuropsychiatry & Clinical Neurosciences, 27(2), 112–120. https://doi.org/http://dx.doi.org/10.1176/appi.neuropsych.13080190
Max, J. E., Pardo, D., Hanten, G., Schachar, R. J., Saunders, A. E., Ewing-Cobbs, L., … Levin, H. S. (2013). Psychiatric disorders in children and adolescents six-to-twelve months after mild traumatic brain injury. Journal of Neuropsychiatry and Clinical Neurosciences, 25(4), 272–282. https://doi.org/http://dx.doi.org/10.1176/appi.neuropsych.12040078
McNally, K. A., Patrick, K. E., LaFleur, J. E., Dykstra, J. B., Monahan, K., & Hoskinson, K. R. (2018). Brief cognitive behavioral intervention for children and adolescents with persistent post-concussive symptoms: A pilot study. Child Neuropsychology, 24(3), 396–412. https://doi.org/10.1080/09297049.2017.1280143
Morgan, C. D., Zuckerman, S. L., Lee, Y. M., King, L., Beaird, S., Sills, A. K., & Solomon, G. S. (2015). Predictors of postconcussion syndrome after sports-related concussion in young athletes: a matched case-control study. Journal of Neurosurgery: Pediatrics, 15(June), 589–598. https://doi.org/10.3171/2014.10.PEDS14356
Mrazik, M., Brooks, B. L., Jubinville, A., Meeuwisse, W. H., & Emery, C. A. (2016). Psychosocial outcomes of sport concussions in youth hockey players. Archives of Clinical Neuropsychology, 31(4), 297–304. https://doi.org/10.1093/arclin/acw013
Nikles, C. J., McKinlay, L., Mitchell, G. K., Carmont, S. A. S., Senior, H. E., Waugh, M. C. A., … Lloyd, O. T. (2014). Aggregated n-of-1 trials of central nervous system stimulants versus placebo for paediatric traumatic brain injury – a pilot study. Trials, 15(1), 1–11. https://doi.org/10.1186/1745-6215-15-54
Peterson, R. L., Connery, A. K., Baker, D. A., & Kirkwood, M. W. (2015). Preinjury Emotional-Behavioral Functioning of Children With Lingering Problems After Mild Traumatic Brain Injury. The Journal of Neuropsychiatry and Clinical Neurosciences, 27(4), 280–286. https://doi.org/10.1176/appi.neuropsych.14120373
Plourde, V., Daya, H., Low, T. A., Barlow, K. M., & Brooks, B. L. (2019). Evaluating anxiety and depression symptoms in children and adolescents with prior mild traumatic brain injury: Agreement between methods and respondents. Child Neuropsychology, 25(1), 44–59. https://doi.org/10.1080/09297049.2018.1432585
Plourde, V., Yeates, K. O., & Brooks, B. L. (2018). Predictors of long-term psychosocial functioning and health-related quality of life in children and adolescents with prior concussions. Journal of the International Neuropsychological Society, 24(6), 540–548. https://doi.org/10.1017/S1355617718000061
Poysophon, P., & Rao, A. L. (2018). Neurocognitive Deficits Associated With ADHD in Athletes: A Systematic Review. Sports Health, 10(4), 317–326. https://doi.org/10.1177/1941738117751387
Reddy, C. C., Collins, M., Lovell, M., & Kontos, A. P. (2013). Efficacy of amantadine treatment on symptoms and neurocognitive performance among adolescents following sports-related concussion. Journal of Head Trauma Rehabilitation, 28(4), 260–265. https://doi.org/10.1097/HTR.0b013e318257fbc6
Rieger, B. P., Lewandowski, L. J., Callahan, J. M., Spenceley, L., Truckenmiller, A., Gathje, R., & Miller, L. A. (2013). A prospective study of symptoms and neurocognitive outcomes in youth with concussion vs orthopaedic injuries. Brain Injury, 27(2), 169–178. https://doi.org/10.3109/02699052.2012.729290
Root, J. M., Zuckerbraun, N. S., Wang, L., Winger, D. G., Brent, D., Kontos, A., & Hickey, R. W. (2016). History of Somatization Is Associated with Prolonged Recovery from Concussion. Journal of Pediatrics, 174, 39–44.e1. https://doi.org/10.1016/j.jpeds.2016.03.020
Ryan, N. P., van Bijnen, L., Catroppa, C., Beauchamp, M. H., Crossley, L., Hearps, S., & Anderson, V. (2016). Longitudinal outcome and recovery of social problems after pediatric traumatic brain injury (TBI): Contribution of brain insult and family environment. International Journal of Developmental Neuroscience, 49, 23–30. https://doi.org/10.1016/j.ijdevneu.2015.12.004
Salinas, C. M., Dean, P., LoGalbo, A., Dougherty, M., Field, M., & Webbe, F. M. (2016). Attention-Deficit Hyperactivity Disorder Status and Baseline Neurocognitive Performance in High School Athletes. Applied Neuropsychology: Child, 5(4), 264–272. https://doi.org/10.1080/21622965.2015.1052814
Segev, S., Shorer, M., Rassovsky, Y., Peleg, T. P., Apter, A., & Fennig, S. (2016). The contribution of posttraumatic stress disorder and mild traumatic brain injury to persistent post concussive symptoms following motor vehicle accidents. Neuropsychology, 30(7), 800–810. https://doi.org/10.1037/neu0000299
Stazyk, K., DeMatteo, C., Moll, S., & Missiuna, C. (2017). Depression in youth recovering from concussion: Correlates and predictors. Brain Injury, 31(5), 631–638. https://doi.org/10.1080/02699052.2017.1283533
Stein, E., Howard, W., Rowhani-Rahbar, A., Rivara, F. P., Zatzick, D., & McCarty, C. A. (2017). Longitudinal trajectories of post-concussive and depressive symptoms in adolescents with prolonged recovery from concussion. Brain Injury, 31(13–14), 1736–1744. https://doi.org/10.1080/02699052.2017.1380843
Truss, K., Godfrey, C., Takagi, M., Babl, F. E., Bressan, S., Hearps, S., … Anderson, V. (2017). Trajectories and Risk Factors for Post-Traumatic Stress Symptoms following Pediatric Concussion. Journal of Neurotrauma, 34(14), 2272–2279. https://doi.org/10.1089/neu.2016.4842
Yang, M. N., Clements-Nolle, K., Parrish, B., & Yang, W. (2019). Adolescent concussion and mental health outcomes: A population-based study. American Journal of Health Behavior, 43(2), 258–265. https://doi.org/10.5993/AJHB.43.2.3
Yengo-Kahn, A. M., & Solomon, G. (2015). Are psychotropic medications associated with differences in baseline neurocognitive assessment scores for young athletes? A pilot study. Physician and Sportsmedicine, 43(3), 227–235. https://doi.org/10.1080/00913847.2015.1071638
Last update: November 16, 2019
 Domain 9: Cognition
Domain 9: Cognition
Introduction:
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
9.1
Evaluate a child/adolescent for cognitive symptoms that interfere with daily functioning following the acute injury.
Level of Evidence: ![]()
For symptoms that interfere with daily functioning for more than 4 weeks following acute injury, further evaluation by experienced professionals to assess cognitive problems may be required.
Depending on the nature of the cognitive symptoms, examples of professionals may include:
- Experienced educational professionals.
- Pediatric neuropsychologists.
- Occupational therapists.
- Speech language pathologists.
Other assessments may be required to determine the underlying cause(s) and any pre-existing contributing factors that can be managed:
- Use a risk score to assess any modifiers that may delay recovery (Recommendation 2.1b).
- A mental health assessment and a closer look at the family may be recommended (Domain 8: Mental Health).
- Vision, vestibular, and hearing assessments may be recommended (Domain 10: Vision, Vestibular, and Oculomotor Function).
- Physical examination (Tool 2.1: Physical Examination).
- As per usual pediatric clinical practice, broad clinical history taking is recommended to understand the youth’s developmental, medical, social, academic, and family histories. Particular consideration should be given to the interplay between these pre-existing factors and current cognitive profile/presentation/symptoms.
9.2
Manage cognitive symptoms that interfere with daily functioning for more than 4 weeks following acute injury.
Level of Evidence: ![]()
See Domain 3: Medical Follow-up and Management of Prolonged Symptoms.
See Domain 12: Return-to-School and Work for suggestions to guide an initial discussion about the best pathways for the student in school, employment, sports, social, and home environments. Tools and tests should be used in conjunction with an examination of previous school records such as marks and teacher observations.
Tools and Resources
- Tool 2.1: Physical Examination
References
Research papers that support the present guideline recommendations:
Babcock, L., Kurowski, B. G., Zhang, N., Dexheimer, J. W., Dyas, J., & Wade, S. L. (2017). Adolescents with Mild Traumatic Brain Injury Get SMART: An Analysis of a Novel Web-Based Intervention. Telemedicine and E-Health, 23(7), 600–607. https://doi.org/10.1089/tmj.2016.0215
Grubenhoff, J. A., Currie, D., Comstock, R. D., Juarez-Colunga, E., Bajaj, L., & Kirkwood, M. W. (2016). Psychological Factors Associated with Delayed Symptom Resolution in Children with Concussion. Journal of Pediatrics, 174(303), 27–32.e1. https://doi.org/10.1016/j.jpeds.2016.03.027
Heyworth, B. E., Carroll, K. M., Rizza, A. J., McInnis, K. C., & Gill, T. J. (2014). Treatment of Concussion in High School Athletes: A Proposed Protocol for Athletic and Academic Return to Activity. Orthopaedic Journal of Sports Medicine, 2(7), 2015. https://doi.org/10.1177/2325967114S00079
McNally, K. A., Patrick, K. E., LaFleur, J. E., Dykstra, J. B., Monahan, K., & Hoskinson, K. R. (2018). Brief cognitive behavioral intervention for children and adolescents with persistent post-concussive symptoms: A pilot study. Child Neuropsychology, 24(3), 396–412. https://doi.org/10.1080/09297049.2017.1280143
Newman, J. B., Reesman, J. H., Vaughan, C. G., & Gioia, G. A. (2013). Assessment of processing speed in children with mild tbi: A “first look” at the validity of pediatric ImPACT. Clinical Neuropsychologist, 27(5), 779–793. https://doi.org/10.1080/13854046.2013.789552
Nikles, C. J., McKinlay, L., Mitchell, G. K., Carmont, S. A. S., Senior, H. E., Waugh, M. C. A., … Lloyd, O. T. (2014). Aggregated n-of-1 trials of central nervous system stimulants versus placebo for paediatric traumatic brain injury – a pilot study. Trials, 15(1), 1–11. https://doi.org/10.1186/1745-6215-15-54
Peltonen, K., Vartiainen, M., Laitala-Leinonen, T., Koskinen, S., Luoto, T., Pertab, J., & Hokkanen, L. (2019). Adolescent athletes with learning disability display atypical maturational trajectories on concussion baseline testing: Implications based on a Finnish sample. Child Neuropsychology, 25(3), 336–351. https://doi.org/10.1080/09297049.2018.1474865
Ransom, D. M., Vaughan, C. G., Pratson, L., Sady, M. D., McGill, C. A., & Gioia, G. A. (2015). Academic Effects of Concussion in Children and Adolescents. Pediatrics, 135(6), 1043–1050. https://doi.org/10.1542/peds.2014-3434
Reddy, C. C., Collins, M., Lovell, M., & Kontos, A. P. (2013). Efficacy of amantadine treatment on symptoms and neurocognitive performance among adolescents following sports-related concussion. Journal of Head Trauma Rehabilitation, 28(4), 260–265. https://doi.org/10.1097/HTR.0b013e318257fbc6
Reed, N., Taha, T., Monette, G., & Keightley, M. (2016). A Preliminary Exploration of Concussion and Strength Performance in Youth Ice Hockey Players. International Journal of Sports Medicine, 37(9), 708–713. https://doi.org/10.1055/s-0042-104199
Taylor, K. M., Kioumourtzoglou, M. A., Clover, J., Coull, B. A., Dennerlein, J. T., Bellinger, D. C., & Weisskopf, M. G. (2018). Concussion History and Cognitive Function in a Large Cohort of Adolescent Athletes. American Journal of Sports Medicine, 46(13), 3262–3270. https://doi.org/10.1177/0363546518798801
Wasserman, E. B., Bazarian, J. J., Mapstone, M., Block, R., & Van Wijngaarden, E. (2016). Academic dysfunction after a concussion among US high school and college students. American Journal of Public Health, 106(7), 1247–1253. https://doi.org/10.2105/AJPH.2016.303154
Last update: November 16, 2019
 Domain 10: Vision, Vestibular and Oculomotor Function
Domain 10: Vision, Vestibular and Oculomotor Function
Introduction:
A repeat medical assessment on concussion patients with prolonged dizziness, blurred or double vision, vertigo, difficulty reading, postural imbalance, or headaches elicited by prolonged visual or vestibular stimulation is required 1-2 weeks following the acute injury. Although the cause of these prolonged symptoms can be multi-factorial, the assessment often reveals impairments in vestibular functioning, balance, or vision. The repeat medical assessment should include a focused clinical history, focused physical examination, and a consideration for the use of additional diagnostic tests as indicated (i.e., screening vestibular oculomotor assessment, visual field testing, and neuroimaging). The medical assessment must consider conditions such as intraparenchymal hemorrhage, stroke, traumatic cranial neuropathy, or temporal bone fractures.
Tool 10.1: Post-Concussion Vestibular (balance/dizziness) and Vision Disturbances Algorithm.
Oculomotor or Vision Deficits
Visual and oculomotor deficits can be due to cranial neuropathies, structural brain injuries, or functional impairments in convergence, accommodation, smooth pursuits, saccades, and vestibulo-ocular reflex functioning. Visual deficits are common symptoms following a concussion. In some patients, these deficits will spontaneously recover and will only need monitoring, supportive care, and anticipatory guidance. However, there is evidence that these deficits may also be associated with increased risk for prolonged symptoms. Identifying these deficits early will allow for early targeted supportive care, management, close monitoring for prolonged, and early referral for further treatment.
Benign Paroxysmal Positional Vertigo
Benign paroxysmal positional vertigo (BPPV) can be caused by the traumatic displacement of the crystals (otoconia) of the inner ear into one of the semi-circular canals. This displacement results in intermittent brief episodes of vertigo and a characteristic pattern of nystagmus (involuntary eye movement) with head movements that stimulate fluid flow in the affected canal (e.g., laying down, sitting up, rolling in bed, looking up, bending over, rapid horizontal head movements). If the patient reports vertigo or dizziness that occurs for seconds following position changes, a screen for BPPV and consideration for targeted particle re-positioning manoeuvres should be conducted. In patients who continue to experience prolonged vertigo or dizziness after completing 3 particle repositioning maneouvers, consideration should be given to a referral to an interdisciplinary concussion team or sub-specialist (i.e., otolaryngology) for further assessment and management.
Vestibulo-Ocular Deficits
The vestibulo-ocular reflex (VOR) enables clear vision with head motion. In many cases, difficulties with clear vision during head motion are reported following a concussion and there is emerging evidence that alterations in VOR function may predict a longer recovery following concussion. Dizziness and/or blurred vision with head motion may be reported and should be further investigated by a healthcare professional with experience in this area. Vestibular rehabilitation has been reported to facilitate recovery when a child/adolescent is experiencing altered gain of the VOR.
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
10.1
Perform a repeat medical assessment on all patients presenting with dizziness, blurred or double vision, vertigo, difficulty reading, postural imbalance, or headaches elicited by prolonged visual or vestibular stimulation 1-2 weeks following acute injury.
Level of Evidence: ![]()
Depending on the nature of the symptoms, the medical assessment should include a focused history, focused physical examination, and consideration for the need for diagnostic brain or cervical spine MRI imaging for those with focal or worrisome symptoms.
Tool 10.1: Post-Concussion Vision, Vestibular, and Oculomotor Disturbances Algorithm.
Tool 2.1: Physical examination.
Recommendation 2.1c: When to consider diagnostic brain or cervical spine imaging.
10.2
Screen for oculomotor or vision deficits.
Level of Evidence: ![]()
Perform an assessment of visual acuity, pupillary function, visual fields, fundoscopy, and extra-ocular movements.
- With appropriate experience, consider an objective assessment of convergence, accommodation, saccades and smooth pursuits.
- Consider additional tests such as automated visual field testing, formal vestibular testing or diagnostic imaging.
Consider referral to an interdisciplinary concussion team or neuro-ophthalmologist, neuro-optometrist, developmental optometrist, occupational therapist, or physiotherapist with competency-based training in vestibular rehabilitation to assess for impairments in convergence, accommodation, saccades and other visual oculomotor disorders.
Online instructional video to consider:
- Link: Visio-Vestibular Examination (The Children’s Hospital of Philadelphia).
10.3
Screen for benign paroxysmal positional vertigo (BPPV) if the patient reports vertigo or dizziness that occurs for seconds following position changes and consider targeted particle re-positioning manoeuvres.
Level of Evidence: ![]()
After completing a neurological screen and clearing the cervical spine to move into the test position, perform the Dix-Hallpike Test. If positive for BPPV (i.e., reproduction of vertigo, typically for seconds, in addition to a characteristic pattern of nystagmus for the canal that is being assessed), a Particle Repositioning Manoeuvre may be appropriate.
Consider the Epley Manoeuvre which can be used to treat the anterior and posterior canals in the case of a canalithiasis. There are many subtypes of BPPV that may require further assessment or alternate canalith repositioning manoeuvres and referral to a healthcare professional (often a physiotherapist with competency-based training in vestibular rehabilitation) for treatment. If symptoms are provoked by pressure (i.e., val salva) or accompanied by a change in hearing, referral to an otolaryngologist or neuro-otologist is warranted.
In patients who continue to experience prolonged vertigo or dizziness despite 3 particle repositioning maneouvers, consider referral to an interdisciplinary concussion team or neuro-otologist or physiotherapist with competency-based training in vestibular rehabilitation. These experienced healthcare professionals should rule out alternative peripheral and central vestibular disorders (e.g., superior semi-circular canal dehiscence (SSCD), vestibular hypofunction) and initiate active management with rehabilitation or referral as appropriate.
Online instructional videos to consider:
- Link: Dix-Hallpike Test (University of Calgary)
- Link: Epley Manoeuvre (University of Calgary)
10.4
Screen for vestibulo-ocular deficits.
Level of Evidence: ![]()
With appropriate experience, perform an assessment of the vestibulo-ocular reflex (VOR) such as the head thrust test and dynamic visual acuity.
Consider referral to a physiotherapist with competency-based training in vestibular rehabilitation.
Online instructional videos to consider:
- Link: Head Thrust Test and Dynamic Visual Acuity (University of Calgary)
- Link: Visio-Vestibular Examination (The Children’s Hospital of Philadelphia)
- Link: Dynamic Visual Acuity (University of Calgary)
10.5
Screen for balance deficits.
Level of Evidence: ![]()
Assess for prolonged balance deficits and determine which systems (visual reflexes, inner ear, musculoskeletal, nervous system or brain) might be contributing to dizziness, headaches, and balance problems. Vestibular rehabilitation may improve balance and dizziness. If prolonged impairment is identified, refer to a specialist immediately.
Perform assessment of postural stability and balance.
- Standing balance test (eyes open/closed, tandem stance, single leg stance), Balance Error Scoring System.
- Dynamic balance: Consider the Functional Gait Assessment and BOT (Bruininks-Oseretsky Test of Motor Proficiency) tests.
Consider referral to an interdisciplinary concussion team or physiotherapist with competency-based training in vestibular rehabilitation.
Online instructional videos to consider:
- Link: Visio-Vestibular Examination (The Children’s Hospital of Philadelphia)
- Link: Balance Error Scoring System (The University of North Carolina at Chapel Hill)
- Link: Functional Gait Assessment (University of Calgary)
10.6
Screen for and consider underlying psychosocial contributors to vestibular, vision, and oculomotor dysfunction.
Level of Evidence: ![]()
Domain 8: Mental Health and Psychosocial Factors.
10.7
Provide general post-concussion education that outlines symptoms of concussion, provides suggestions regarding activity modification and includes academic accommodations to manage visual, vestibular and oculomotor symptoms.
Level of Evidence: ![]()
Guidance about how to make a gradual return-to-school, cognitive activities, and physical activities:
- Recommendation 2.3: Recommend graduated return to cognitive and physical activity.
- Recommendation 2.4c: Advise on the use of computers, phones, and other screen devices.
- Domain 12: Return-to-School and Work.
10.8
Encourage patients with post-concussion vestibular, visual, or oculomotor symptoms to engage in cognitive activity and low-risk physical activity as soon as tolerated while staying below their symptom-exacerbation thresholds. Activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) should be resumed even if mild residual symptoms are present or whenever acute symptoms improve sufficiently to permit activity.
Level of Evidence: ![]() Gradual return to physical activity.
Gradual return to physical activity. ![]() Gradual return to cognitive activity.
Gradual return to cognitive activity.
See Recommendation 2.3.
- Refer select patients (e.g., highly-active or competitive athletes, those who are not tolerating a graduated return to physical activity, or those who are slow to recover) following acute injury to a medically supervised interdisciplinary team with the ability to individually assess sub-symptom threshold aerobic exercise tolerance and to prescribe aerobic exercise treatment. This exercise tolerance assessment can be as early as 48 hours following acute injury. Level of Evidence:

- Patients who are active may benefit from referral to a medically supervised interdisciplinary team with the ability to individually assess sub-symptom threshold aerobic exercise tolerance and to prescribe aerobic exercise treatment. This exercise tolerance assessment can be as early as 48 hours following acute injury. Level of Evidence:

See Tool 2.6: Post-Concussion Information Sheet for examples of low-risk activities.
10.9
Refer patients with prolonged post-concussion vestibular functioning, balance or visual dysfunction (more than 4 weeks following the acute injury) to an interdisciplinary concussion team with appropriate experience. Consider early referral (before 4 weeks) to an interdisciplinary concussion team in the presence of modifiers that may delay recovery.
Level of Evidence: ![]() Medical follow-up.
Medical follow-up. ![]() Early referral in the presence of modifiers that may delay recovery.
Early referral in the presence of modifiers that may delay recovery.
Specialized interdisciplinary concussion care is ideally initiated for patients at elevated risk for a delayed recovery within the first two weeks post-injury. Level of Evidence: ![]()
Tool 10.1: Post-Concussion Vision, Vestibular, and Oculomotor Disturbances Algorithm
Assessment by an interdisciplinary concussion team can assist in identifying the type of management that is required, along with the medical and health professions on the interdisciplinary concussion team or external to this team who can provide the required management. Not all children/adolescents will require care from all members of the interdisciplinary concussion team and care should be targeted based on identified symptoms and patient needs.
See Recommendation 2.1b: Note any modifiers that may delay recovery and use a clinical risk score to predict risk of prolonged symptoms.
10.10
Recommend a medical follow-up to reassess clinical status if vestibular functioning, balance or visual dysfunction symptoms persist. Recommend an immediate medical follow-up in the presence of any deterioration.
Level of Evidence: ![]()
Tools and Resources
- Tool 2.1: Physical Examination
- Tool 2.6: Post-Concussion Information Sheet
- Tool 10.1: Post-Concussion Vestibular (balance/dizziness) and Vision Disturbances Algorithm
Online videos to consider:
- Dix-Hallpike Test (University of Calgary)
- Epley Manoeuvre (University of Calgary)
- Head Thrust Test and Dynamic Visual Acuity (University of Calgary)
- Visio-Vestibular Examination (The Children’s Hospital of Philadelphia)
- Balance Error Scoring System (The University of North Carolina at Chapel Hill)
References
Click here to access the Living Guideline Evidence Map (powered by EPPIreviewer and EPPIvisualizer)
Reference List: Last updated Sept 2023, update in progress (April 2024).
ALBERTS JAY L, THOTA ANIL, HIRSCH JOSHUA, OZINGA SARAH, DEY TANUJIT, SCHINDLER DAVID D, KOOP MANDY M, BURKE DANIEL, and LINDER SUSAN M (2015) Quantification of the Balance Error Scoring System with Mobile Technology. Medicine & Science in Sports & Exercise 47(10), 2233-2240 DOI: 10.1249/MSS.0000000000000656
Albrecht Ted J, Makwana Mehmel Bindal, Rossi Ethan A, Trbovich Alicia M, Eagle Shawn R, and Kontos Anthony P (2024) Temporal Changes in Fixational Eye Movements After Concussion in Adolescents and Adults: Preliminary Findings. Journal of Neurotrauma 41(1-2), 199-208
Alexander Amy, Hattrup Nicholas, Gerkin Richard, and Pardini Jamie E (2022) Gaze stability in youth athletes: A normative observational study. Journal of vestibular research : equilibrium & orientation 32(6), 511-515
Alkathiry Abdulaziz A, Kontos Anthony P, Furman Joseph M, Whitney Susan L, Anson Eric R, and Sparto Patrick J (2019) Vestibulo-Ocular Reflex Function in Adolescents With Sport-Related Concussion: Preliminary Results. Sports Health 11(6), 479-485 DOI: 10.1177/1941738119865262
Alkathiry Abdulaziz A, Alsubaie Saud F, Alsalaheen Bara A, and Whitney Susan L (2022) Validation of the Gait Disorientation Test in children with concussion. Frontiers in Pediatrics 10, 927708
Alsalaheen Bara A, Haines Jamie, Yorke Amy, Stockdale Kayla, and Broglio Steven P (2015) Reliability and concurrent validity of instrumented balance error scoring system using a portable force plate system. Physician and Sportsmedicine 43(3), 221-226 DOI: 10.1080/00913847.2015.1040717
Alsalaheen Bara, McClafferty Adam, Haines Jamie, Smith Laura, and Yorke Amy (2016) Reference values for the balance error scoring system in adolescents. Brain Injury 30(7), 914-918 DOI: 10.3109/02699052.2016.1146965
Alsalaheen Bara A, Whitney Susan L, Marchetti Gregory F, Furman Joseph M, Kontos Anthony P, Collins Michael W, and Sparto Patrick J (2016) Relationship between cognitive assessment and balance measures in adolescents referred for vestibular physical therapy after concussion. Clinical Journal of Sport Medicine 26(1), 46-52 DOI: 10.1097/JSM.0000000000000185
Alsalaheen Bara, Carender Wendy, Grzesiak Melissa, Munday Cindy, Almeida Andrea, Lorincz Matthew, and Marchetti Gregory F (2020) Changes in Vestibular/Ocular-Motor Screen Scores in Adolescents Treated With Vestibular Therapy After Concussion. Pediatric physical therapy : the official publication of the Section on Pediatrics of the American Physical Therapy Association 32(4), 331-337
Anderson Stevi L, Gatens Dustin, Glatts Colette, and Russo Stephen A (2019) Normative Data Set of SWAY Balance Mobile Assessment in Pediatric Athletes. Clinical Journal of Sport Medicine 29(5), 413-420 DOI: 10.1097/JSM.0000000000000545
Anzalone Anthony J, Blueitt Damond, Case Tami, McGuffin Tiffany, Pollard Kalyssa, Garrison J Craig, Jones Margaret T, Pavur Robert, Turner Stephanie, and Oliver Jonathan M (2017) A Positive Vestibular/Ocular Motor Screening (VOMS) Is Associated with Increased Recovery Time after Sports-Related Concussion in Youth and Adolescent Athletes. American Journal of Sports Medicine 45(2), 474-479 DOI: 10.1177/0363546516668624
Arbogast Kristy B, Ghosh Riddhi P, Corwin Daniel J, McDonald Catherine C, Mohammed Fairuz N, Margulies Susan S, Barnett Ian, and Master Christina L (2022) Trajectories of Visual and Vestibular Markers of Youth Concussion. Journal of Neurotrauma 39(19-20), 1382-1390
Babicz Michelle A, Woods Steven Paul, Cirino Paul, Presley Chase, Colton Zachary, and Podell Kenneth (2022) Vestibular/Ocular Motor Screening is Independently Associated With Concussion Symptom Severity in Youths. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 32(1), 40-45
Barnes Alice, Smulligan Katherine, Wingerson Mathew J, Little Casey, Lugade Vipul, Wilson Julie C, and Howell David R (2024) A Multifaceted Approach to Interpreting Reaction Time Deficits After Adolescent Concussion. Journal of Athletic Training 59(2), 145-152
Białuńska Anita, and Salvatore Anthony P (2017) The auditory comprehension changes over time after sport-related concussion can indicate multisensory processing dysfunctions. Brain and Behavior 7(12), 1-8 DOI: 10.1002/brb3.874
Brett Benjamin L, Zuckerman Scott L, Terry Douglas P, Solomon Gary S, and Iverson Grant L (2018) Normative Data for the Sway Balance System. Clinical Journal of Sport Medicine (00), 1-1 DOI: 10.1097/jsm.0000000000000632
Chinn Ryan N, Marusic Sophia, Wang Alicia, Vyas Neerali, Staffa Steven J, Brodsky Jacob R, and Raghuram Aparna (2022) Vergence and Accommodation Deficits in Children and Adolescents with Vestibular Disorders. Optometry and vision science : official publication of the American Academy of Optometry 99(12), 859-867
Conder Robert L, Conder Alanna A, Register-Mihalik Johna, Conder Lauren H, and Newton Shannon (2015) Preliminary Normative Data on the Penn State University Symbol Cancellation Task With Nonconcussed Adolescents. Applied Neuropsychology: Child 4(3), 141-147 DOI: 10.1080/21622965.2013.816849
Corwin Daniel J, Wiebe Douglas J, Zonfrillo Mark R, Grady Matthew F, Robinson Roni L, Goodman Arlene M, and Master Christina L (2015) Vestibular Deficits following Youth Concussion. The Journal of Pediatrics 166(5), 1221-1225 DOI: 10.1016/j.jpeds.2015.01.039
Corwin Daniel J, Zonfrillo Mark R, Wiebe Douglas J, Master Christina L, Grady Matthew F, and Arbogast Kristy B (2018) Vestibular and oculomotor findings in neurologically-normal, non-concussed children. Brain Injury 32(6), 794-799 DOI: 10.1080/02699052.2018.1458150
Corwin Daniel J, Propert Kathleen J, Zorc Joseph J, Zonfrillo Mark R, and Wiebe Douglas J (2019) Use of the vestibular and oculomotor examination for concussion in a pediatric emergency department. American Journal of Emergency Medicine 37(7), 1219-1223 DOI: 10.1016/j.ajem.2018.09.008
Corwin Daniel J, McDonald Catherine C, Arbogast Kristy B, Mohammed Fairuz N, Metzger Kristina B, Pfeiffer Melissa R, Patton Declan A, Huber Colin M, Margulies Susan S, Grady Matthew F, and Master Christina L (2020) Clinical and Device-based Metrics of Gait and Balance in Diagnosing Youth Concussion. Medicine and science in sports and exercise 52(3), 542-548
Corwin Daniel J, Arbogast Kristy B, Swann Casey, Haber Rebecca, Grady Matthew F, and Master Christina L (2020) Reliability of the visio-vestibular examination for concussion among providers in a pediatric emergency department. American Journal of Emergency Medicine 38(9), 1847-1853 DOI: 10.1016/j.ajem.2020.06.020
Corwin Daniel J, McDonald Catherine C, Arbogast Kristy B, Mohammed Fairuz N, Grady Matthew F, and Master Christina L (2021) Visio-Vestibular Deficits in Healthy Child and Adolescent Athletes. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine ,
Crampton Adrienne, Schneider Kathryn J, Grilli Lisa, Chevignard Mathilde, Katz-Leurer Michal, Beauchamp Miriam H, Debert Chantel, and Gagnon Isabelle J (2022) Characterizing the evolution of oculomotor and vestibulo-ocular function over time in children and adolescents after a mild traumatic brain injury. Frontiers in Neurology 13, 904593
Crampton Adrienne, Schneider Kathryn J, Grilli Lisa, Chevignard Mathilde, Katz-Leurer Michal, Beauchamp Miriam H, Debert Chantel, and Gagnon Isabelle J (2022) Determining the Agreement Between Common Measures Related to Vestibulo-ocular Reflex Function After a Mild Traumatic Brain Injury in Children and Adolescents. Archives of rehabilitation research and clinical translation 4(3), 100217
Del Rossi Gianluca (2022) Examination of Near Point of Convergence Scores in High-School Athletes: Implications for Identifying Binocular Vision Dysfunction After Concussion Injury. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 32(5), e451-e456
Donner Julia R, Corwin Daniel J, Master Christina L, and Zonfrillo Mark R (2022) Documented Visio-Vestibular Examination and Anticipatory Guidance for Pediatric Concussion Patients. Pediatric Emergency Care ,
Dorman Jason C, Valentine Verle D, Munce Thayne A, Tjarks B Joel, Thompson Paul A, and Bergeron Michael F (2015) Tracking postural stability of young concussion patients using dual-task interference. Journal of Science and Medicine in Sport 18(1), 2-7 DOI: 10.1016/j.jsams.2013.11.010
Eagle Shawn R, Sparto Patrick J, Holland Cynthia L, Alkathiry Abdulaziz A, Blaney Nicholas A, Bitzer Hannah B, Collins Michael W, Furman Joseph M, and Kontos Anthony P (2021) Utility of a Postural Stability/Perceptual Inhibition Dual Task for Identifying Concussion in Adolescents. Journal of Sport Rehabilitation , 1-6
Eagle Shawn R, Feder Abigail, Manderino Lisa M, Mucha Anne, Holland Cyndi L, Collins Michael W, and Kontos Anthony P (2022) Concurrent validity of the Vestibular/Ocular Motor Screening (VOMS) tool with the Dizziness Handicap Inventory (DHI) among adolescents with vestibular symptoms/impairment following concussion. Physical therapy in sport : official journal of the Association of Chartered Physiotherapists in Sports Medicine 53, 34-39
Elbin R J, Eagle Shawn R, Marchetti Gregory F, Anderson Morgan, Schatz Philip, Womble Melissa N, Stephenson Katie, Covassin Tracey, Collins Michael W, Mucha Anne, and Kontos Anthony P (2021) Using change scores on the vestibular ocular motor screening (VOMS) tool to identify concussion in adolescents. Applied neuropsychology.Child , 1-7
Ellis Michael J, Cordingley Dean, Vis Sara, Reimer Karen, Leiter Jeff, and Russell Kelly (2015) Vestibulo-ocular dysfunction in pediatric sports-related concussion. Journal of Neurosurgery: Pediatrics 16(3), 248-255 DOI: 10.3171/2015.1.PEDS14524
Ellis Michael J, Cordingley Dean M, Vis Sara, Reimer Karen M, Leiter Jeff, and Russell Kelly (2017) Clinical predictors of vestibulo-ocular dysfunction in pediatric sports-related concussion. Journal of Neurosurgery: Pediatrics 19(1), 38-45 DOI: 10.3171/2016.7.PEDS16310
Erdman Nicholas K, Kelshaw Patricia M, Hacherl Samantha L, and Caswell Shane V (2023) Footwear Type and Testing Environment Do Not Affect Baseline Modified Balance Error Scoring System Performance Among Middle School Athletes. Journal of Sport Rehabilitation 32(1), 9-13
Ernst Nathan, Schatz Philip, Trbovich Alicia M, Emami Kouros, Eagle Shawn R, Mucha Anne, Collins Michael W, and Kontos Anthony P (2020) Utility of 1 Measurement Versus Multiple Measurements of Near Point of Convergence After Concussion. Journal of Athletic Training 55(8), 850-855
Fino Peter C, Nussbaum Maury A, and Brolinson Per Gunnar (2016) Locomotor deficits in recently concussed athletes and matched controls during single and dual-task turning gait: Preliminary results. Journal of NeuroEngineering and Rehabilitation 13(1), 1-15 DOI: 10.1186/s12984-016-0177-y
Fino Peter C (2016) A preliminary study of longitudinal differences in local dynamic stability between recently concussed and healthy athletes during single and dual-task gait. Journal of Biomechanics 49(9), 1983-1988 DOI: 10.1016/j.jbiomech.2016.05.004
Furman Gabriel R, Lin Chia Cheng, Bellanca Jennica L, Marchetti Gregory F, Collins Michael W, and Whitney Susan L (2013) Comparison of the balance accelerometer measure and balance error scoring system in adolescent concussions in sports. American Journal of Sports Medicine 41(6), 1404-1410 DOI: 10.1177/0363546513484446
Galetta Kristin M, Morganroth Jennifer, Moehringer Nicholas, Mueller Bridget, Hasanaj Lisena, Webb Nikki, Civitano Courtney, Cardone Dennis A, Silverio Arlene, Galetta Steven L, and Balcer Laura J (2015) Adding vision to concussion testing: A prospective study of sideline testing in youth and collegiate athletes. Journal of Neuro-Ophthalmology 35(3), 235-241 DOI: 10.1097/WNO.0000000000000226
Gowrisankaran Sowjanya, Shah Ankoor S, Roberts Tawna L, Wiecek Emily, Chinn Ryan N, Hawash Karameh K, O’Brien Michael J, Howell David R, Meehan William P, and Raghuram Aparna (2021) Association between post-concussion symptoms and oculomotor deficits among adolescents. Brain Injury , 1-11
Gray Margot, Wilson Julie C, Potter Morgan, Provance Aaron J, and Howell David R (2020) Female adolescents demonstrate greater oculomotor and vestibular dysfunction than male adolescents following concussion. Physical therapy in sport : official journal of the Association of Chartered Physiotherapists in Sports Medicine 42, 68-74
Haider M Nadir, Patel Kush S, Willer Barry S, Videira Victoria, Wilber Charles G, Mayer Andrew R, Master Christina L, Mariotti Brandon L, Wertz Christopher, Storey Eileen P, Arbogast Kristy B, Park Grace, Oglesbee Scott J, Bezherano Itai, Aguirre Kenneth, Fodero Jesse G, Johnson Blair D, Mannix Rebekah, Miecznikowski Jeffrey C, and Leddy John J (2021) Symptoms upon postural change and orthostatic hypotension in adolescents with concussion. Brain Injury 35(2), 226-232
Hansen Colby, Cushman Dan, Anderson Nicholas, Chen Wei, Cheng Christine, Hon Shirley D, and Hung Man (2016) A Normative Dataset of the Balance Error Scoring System in Children Aged between 5 and 14. Clinical Journal of Sport Medicine 26(6), 497-501 DOI: 10.1097/JSM.0000000000000285
Hansen Colby, Cushman Dan, Chen Wei, Bounsanga Jerry, and Hung Man (2017) Reliability testing of the balance error scoring system in children between the ages of 5 and 14. Clinical Journal of Sport Medicine 27(1), 64-68 DOI: 10.1097/JSM.0000000000000293
Heyer Geoffrey L, Young Julie A, and Fischer Anastasia N (2017) Lightheadedness After Concussion: Not All Dizziness is Vertigo. Clinical Journal of Sport Medicine 0(0), DOI: 10.1097/JSM.0000000000000445
Howell David R, Osternig Louis R, and Chou Li Shan (2013) Dual-task effect on gait balance control in adolescents with concussion. Archives of Physical Medicine and Rehabilitation 94(8), 1513-1520 DOI: http://dx.doi.org/10.1016/j.apmr.2013.04.015
Howell David R, Osternig Louis R, Koester Michael C, and Chou Li-Shan (2014) The effect of cognitive task complexity on gait stability in adolescents following concussion. Experimental Brain Research 232(6), 1773-1782 DOI: 10.1007/s00221-014-3869-1
Howell David R, Osternig Louis R, and Chou Li Shan (2015) Adolescents demonstrate greater gait balance control deficits after concussion than young adults. American Journal of Sports Medicine 43(3), 625-632 DOI: 10.1177/0363546514560994
Howell David R, Osternig Louis R, and Chou Li Shan (2015) Return to activity after concussion affects dual-task gait balance control recovery. Medicine and Science in Sports and Exercise 47(4), 673-680 DOI: 10.1249/MSS.0000000000000462
Howell David R, Osternig Louis R, and Chou Li Shan (2016) Consistency and cost of dual-task gait balance measure in healthy adolescents and young adults. Gait and Posture 49, 176-180 DOI: 10.1016/j.gaitpost.2016.07.008
Howell David R, Shore Benjamin J, Hanson Emily, and Meehan William P (2016) Evaluation of postural stability in youth athletes: the relationship between two rating systems. Physician and Sportsmedicine 44(3), 304-310 DOI: 10.1080/00913847.2016.1197763
Howell David R, Stracciolini Andrea, Geminiani Ellen, and Meehan William P (2017) Dual-task gait differences in female and male adolescents following sport-related concussion. Gait and Posture 54(November 2016), 284-289 DOI: 10.1016/j.gaitpost.2017.03.034
Howell David R, Brilliant Anna, Berkstresser Brant, Wang Francis, Fraser Joana, and Meehan William P (2017) The Association between Dual-Task Gait after Concussion and Prolonged Symptom Duration. Journal of Neurotrauma 34(23), 3288-3294 DOI: 10.1089/neu.2017.5191
Howell David R, OʼBrien Michael J, Raghuram Aparna, Shah Ankoor S, and Meehan William P (2017) Near Point of Convergence and Gait Deficits in Adolescents After Sport-Related Concussion. Clinical Journal of Sport Medicine 0(0), DOI: 10.1097/JSM.0000000000000439
Howell David R, Hanson Emily, Sugimoto Dai, Stracciolini Andrea, and Meehan William P (2017) Assessment of the Postural Stability of Female and Male Athletes. Clinical Journal of Sport Medicine 27(5), 444-449 DOI: 10.1097/JSM.0000000000000374
Howell David R, Beasley Michael, Vopat Lisa, and Meehan William P (2017) The Effect of Prior Concussion History on Dual-Task Gait following a Concussion. Journal of Neurotrauma 34(4), 838-844 DOI: 10.1089/neu.2016.4609
Howell David R, Brilliant Anna N, Storey Eileen P, Podolak Olivia E, Meehan William P. 3rd, and Master Christina L (2018) Objective Eye Tracking Deficits Following Concussion for Youth Seen in a Sports Medicine Setting. Journal of Child Neurology 33(12), 794-800 DOI: 10.1177/0883073818789320
Howell David R, Lugade Vipul, Potter Morgan N, Walker Gregory, and Wilson Julie C (2019) A multifaceted and clinically viable paradigm to quantify postural control impairments among adolescents with concussion. Physiological Measurement 40(8), DOI: 10.1088/1361-6579/ab3552
Howell David R, Myer Gregory D, Grooms Dustin, Diekfuss Jed, Yuan Weihong, and Meehan William P. 3rd (2019) Examining Motor Tasks of Differing Complexity After Concussion in Adolescents.. Archives of Physical Medicine and Rehabilitation 100(4), 613-619 DOI: 10.1016/j.apmr.2018.07.441
Howell David R, Bonnette Scott, Diekfuss Jed A, Grooms Dustin R, Myer Gregory D, and Meehan William P (2020) Youth With Concussion Have Less Adaptable Gait Patterns Than Their Uninjured Peers: Implications for Concussion Management. The Journal of orthopaedic and sports physical therapy 50(8), 438-446
Hsu Jerry, Stec Magdalena, Ranaivo Hantamalala Ralay, Srdanovic Nina, and Kurup Sudhi P (2020) Concussion Alters Dynamic Pupillary Light Responses in Children. Journal of Child Neurology , 883073820964040
Hugentobler Jason A, Gupta Resmi, Slater Robert, Paterno Mark V, Riley Michael A, and Quatman-Yates Catherine (2016) Influence of Age on Postconcussive Postural Control Measures and Future Implications for Assessment. Clinical Journal of Sport Medicine 26(6), 510-517 DOI: 10.1097/JSM.0000000000000286
Hunfalvay Melissa, Murray Nicholas P, Roberts Claire Marie, Tyagi Ankur, Barclay Kyle William, and Carrick Frederick Robert (2020) Oculomotor Behavior as a Biomarker for Differentiating Pediatric Patients With Mild Traumatic Brain Injury and Age Matched Controls. Frontiers in behavioral neuroscience 14, 581819
Hunfalvay Melissa, Murray Nicholas P, and Carrick Frederick Robert (2021) Fixation stability as a biomarker for differentiating mild traumatic brain injury from age matched controls in pediatrics. Brain Injury 35(2), 209-214
Hunfalvay Melissa, Murray Nicholas P, Mani Revathy, and Carrick Frederick Robert (2021) Smooth Pursuit Eye Movements as a Biomarker for Mild Concussion within 7-Days of Injury. Brain Injury 35(14), 1682-1689
Hunt Danielle L, Oldham Jessie, Aaron Stacey E, Tan Can Ozan, Meehan William P, and Howell David R (2022) Dizziness, Psychosocial Function, and Postural Stability Following Sport-Related Concussion. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 32(4), 361-367
Jain Divya, Arbogast Kristy B, McDonald Catherine C, Podolak Olivia E, Margulies Susan S, Metzger Kristina B, Howell David R, Scheiman Mitchell M, and Master Christina L (2022) Eye Tracking Metrics Differences among Uninjured Adolescents and Those with Acute or Persistent Post-Concussion Symptoms. Optometry and vision science : official publication of the American Academy of Optometry 99(8), 616-625
King Laurie A, Horak Fay B, Mancini Martina, Pierce Donald, Priest Kelsey C, Chesnutt James, Sullivan Patrick, and Chapman Julie C (2014) Instrumenting the balance error scoring system for use with patients reporting persistent balance problems after mild traumatic brain injury. Archives of Physical Medicine and Rehabilitation 95(2), 353-359 DOI: 10.1016/j.apmr.2013.10.015
Knell Gregory, Caze Todd, and Burkhart Scott O (2021) Evaluation of the vestibular and ocular motor screening (VOMS) as a prognostic tool for protracted recovery following paediatric sports-related concussion. BMJ Open Sport & Exercise Medicine 7(1), e000970
Königs Marsh, Weeda Wouter D, Van Heurn L W.Ernest, Vermeulen R Jeroen, Goslings J Carel, Luitse Jan S.K, Poll-Thé Bwee Tien, Beelen Anita, Van Der Wees Marleen, Kemps Rachèl J.J.K, Catsman-Berrevoets Coriene E, and Oosterlaan Jaap (2015) Impaired Visual Integration in Children with Traumatic Brain Injury: An Observational Study. PLoS ONE 10(12), 1-15 DOI: 10.1371/journal.pone.0144395
Kontos Anthony P, Eagle Shawn R, Mucha Anne, Kochick Victoria, Reichard Jessica, Moldolvan Claire, Holland Cyndi L, Blaney Nicholas A, and Collins Michael W (2021) A Randomized Controlled Trial of Precision Vestibular Rehabilitation in Adolescents following Concussion: Preliminary Findings. The Journal of Pediatrics ,
Kraus Nina, Thompson Elaine C, Krizman Jennifer, Cook Katherine, White-Schwoch Travis, and LaBella Cynthia R (2016) Auditory biological marker of concussion in children. Scientific Reports 6(August), 1-10 DOI: 10.1038/srep39009
Leonard Bianca T, Kontos Anthony P, Marchetti Gregory F, Zhang Min, Eagle Shawn R, Reecher Hope M, Bensinger Ethan S, Snyder Valerie C, Holland Cyndi L, Sheehy Christy K, and Rossi Ethan A (2021) Fixational eye movements following concussion. Journal of vision 21(13), 11
Leung Felix T, Mendis M Dilani, Franettovich Smith Melinda M, Rahmann Ann, Treleaven Julia, and Hides Julie A (2022) Sensorimotor system changes in adolescent rugby players post-concussion: A prospective investigation from the subacute period through to return-to-sport. Musculoskeletal Science & Practice 57, 102492
Linder Susan M, Ozinga Sarah J, Koop Mandy Miller, Dey Tanujit, Figler Richard, Cruickshank Jason, and Alberts Jay L (2018) Cleveland Clinic Postural Stability Index Norms for the Balance Error Scoring System. Medicine and Science in Sports and Exercise 50(10), 1998-2006 DOI: 10.1249/MSS.0000000000001660
Lowe Leah, Castillo Fernando, Gokun Yevgeniya, Williams David K, Israel Michael, and Yates Charlotte (2022) Static and Dynamic Balance Assessment in Healthy and Concussed Adolescent Athletes. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 32(4), 385-390
Manaseer Thaer S, Gross Douglas P, Dennett Liz, Schneider Kathryn, and Whittaker Jackie L (2020) Gait Deviations Associated With Concussion: A Systematic Review. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 30 Suppl 1, S11-S28
Mang Cameron S, Whitten Tara A, Cosh Madeline S, Dukelow Sean P, and Benson Brian W (2020) Assessment of Postural Stability During an Upper Extremity Rapid, Bimanual Motor Task After Sport-Related Concussion. Journal of Athletic Training 55(11), 1160-1173
Mani Revathy, Ngo Steven, Walz Jacinta, and Khuu Sieu K (2022) Evaluating the extent of change in near point of convergence in traumatic brain injury: a systematic review and meta-analysis. Brain Injury 36(3), 306-320
Master Christina L, Scheiman Mitchell, Gallaway Michael, Goodman Arlene, Robinson Roni L, Master Stephen R, and Grady Matthew F (2016) Vision Diagnoses Are Common after Concussion in Adolescents. Clinical Pediatrics 55(3), 260-267 DOI: 10.1177/0009922815594367
Master Christina L, Master Stephen R, Wiebe Douglas J, Storey Eileen P, Lockyer Julia E, Podolak Olivia E, and Grady Matthew F (2018) Vision and Vestibular System Dysfunction Predicts Prolonged Concussion Recovery in Children. Clinical Journal of Sport Medicine 28(2), 139-145 DOI: 10.1097/JSM.0000000000000507
Master Christina L, Curry Allison E, Pfeiffer Melissa R, Metzger Kristina B, Kessler Ronni S, Haarbauer-Krupa Juliet, DePadilla Lara, Greenspan Arlene, Breiding Matthew J, and Arbogast Kristy B (2020) Characteristics of Concussion in Elementary School-Aged Children: Implications for Clinical Management. Journal of Pediatrics 223, 128-135 DOI: 10.1016/j.jpeds.2020.04.001
Mayer Andrew R, Wertz Christopher J, Robertson-Benta Cidney R, Pabbathi Reddy Sharvani, Stephenson David D, Dodd Andrew B, Oglesbee Scott J, Bedrick Edward J, Master Christina L, Grady Mathew, Shaff Nicholas A, Hanlon Faith M, Campbell Richard A, Phillips John P, Zemek Roger L, Yeates Keith Owen, Meier Timothy B, Mannix Rebekah, Leddy John J, Arbogast Kristy B, and Park Grace (2020) Neurosensory Screening and Symptom Provocation in Pediatric Mild Traumatic Brain Injury. The Journal of head trauma rehabilitation 35(4), 270-278
Moran Ryan N, and Bretzin Abigail C (2023) Long-term test-retest reliability of the vestibular/ocular motor screening for concussion in child athletes: A preliminary study. Applied neuropsychology.Child , 1-6
Mucha Anne, Collins Michael W, Elbin R J, Furman Joseph M, Troutman-Enseki Cara, DeWolf Ryan M, Marchetti Greg, and Kontos Anthony P (2014) A Brief Vestibular/Ocular Motor Screening (VOMS) Assessment to Evaluate Concussions. The American Journal of Sports Medicine 42(10), 2479-2486 DOI: 10.1177/0363546514543775
Murray Nicholas G, Ambati V N. Pradeep, Contreras Monica M, Salvatore Anthony P, and Reed-Jones Rebecca J (2014) Assessment of oculomotor control and balance post-concussion: A preliminary study for a novel approach to concussion management. Brain Injury 28(4), 496-503 DOI: 10.3109/02699052.2014.887144
Oldham Jessie R, Meehan William P, and Howell David R (2021) Impaired eye tracking is associated with symptom severity but not dynamic postural control in adolescents following concussion. Journal of sport and health science 10(2), 138-144
Ozinga Sarah J, Linder Susan M, Koop Mandy Miller, Dey Tanujit, Figler Richard, Russman Andrew N, So Richard, Rosenthal Alan H, Cruickshank Jason, and Alberts Jay L (2018) Normative performance on the balance error scoring system by youth, high school, and collegiate athletes. Journal of Athletic Training 53(7), 636-645 DOI: 10.4085/1062-6050-129-17
Patel Rishi D, and LaBella Cynthia R (2021) Contributions of PCSS, BESS, Tandem Gait, and Romberg Test for Identifying Balance Deficits in Pediatric Concussions. The Journal of head trauma rehabilitation ,
Pavlou Marousa, Whitney Susan L, Alkathiry Abdulaziz A, Huett Marian, Luxon Linda M, Raglan Ewa, Godfrey Emma L, and Bamiou Doris Eva (2017) Visually induced dizziness in children and validation of the Pediatric Visually Induced Dizziness Questionnaire. Frontiers in Neurology 8(DEC), 1-9 DOI: 10.3389/fneur.2017.00656
Pearce Kelly L, Sufrinko Alicia, Lau Brian C, Henry Luke, Collins Michael W, and Kontos Anthony P (2015) Near Point of Convergence After a Sport-Related Concussion. The American Journal of Sports Medicine 43(12), 3055-3061 DOI: 10.1177/0363546515606430
Pearce Alan J, Daly Ed, Ryan Lisa, and King Doug (2023) Reliability of a Smooth Pursuit Eye-Tracking System (EyeGuide Focus) in Healthy Adolescents and Adults. Journal of functional morphology and kinesiology 8(2),
Peiffer Adam J, MacDonald James, Duerson Drew, Mitchell Gladys, Hartwick Andrew T.E, and McDaniel Catherine E (2020) The Influence of Binocular Vision Symptoms on Computerized Neurocognitive Testing of Adolescents With Concussion. Clinical Pediatrics 59(11), 961-969
Phillips Brandon, Adkins Jaxon C, Jones Briasha D, and Dalecki Marc (2023) Prolonged eye-hand decoupling deficits in young adults with a history of concussion from adolescence. European Journal of Sport Science 23(6), 1036-1046
Pieniak Michal, Seidel Katharina, Oleszkiewicz Anna, Gellrich Janine, Karpinski Christian, Fitze Guido, and Schriever Valentin A (2023) Olfactory training effects in children after mild traumatic brain injury. Brain Injury 37(11), 1272-1284
Popovich Michael, Almeida Andrea, Lorincz Matthew, Eckner James T, Freeman Jeremiah, Streicher Nicholas, and Alsalaheen Bara (2021) Does Exercise Increase Vestibular and Ocular Motor Symptom Detection After Sport-Related Concussion?. Journal of neurologic physical therapy : JNPT 45(3), 214-220
Preszler Jonathan, Manderino Lisa, Fazio-Sumrok Vanessa, Eagle Shawn R, Holland Cynthia, Collins Michael W, and Kontos Anthony P (2022) Multidomain concussion symptoms in adolescents: A network analysis. Applied neuropsychology.Child , 1-10
Price August M, Knell Gregory, Caze Todd J, Abt John P, Loveland Dustin, and Burkhart Scott O (2022) Exploring Vestibular/Ocular and Cognitive Dysfunction as Prognostic Factors for Protracted Recovery in Sports-Related Concussion Patients Aged 8 to 12 Years. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine 32(4), 408-414
Quatman-Yates Catherine, Hugentobler Jason, Ammon Robin, Mwase Najima, Kurowski Brad, and Myer Gregory D (2014) The utility of the balance error scoring system for mild brain injury assessments in children and adolescents. Physician and Sportsmedicine 42(3), 32-38 DOI: 10.3810/psm.2014.09.2073
 Domain 11: Fatigue
Domain 11: Fatigue
Introduction:
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
11.1
Perform a repeat medical assessment on all patients presenting with post-concussion fatigue 1-2 weeks following acute injury.
Level of Evidence: ![]()
The medical assessment should include a clinical history of symptoms, physical examination, and screen for other causes of fatigue (e.g., mononucleosis, anemia, thyroid dysfunction, mood disorders, pregnancy, etc.).
11.2
Provide patients with post-concussion fatigue with general education and guidance that outlines non-pharmacological strategies to help cope with fatigue symptoms and set expectations.
Level of Evidence: ![]()
Strategies and post-concussion education guidance related to fatigue:
- Emphasize that spreading activities throughout the day helps patients achieve more and that they should avoid doing too much at once.
- Encourage good diet and hydration.
- Encourage good sleep hygiene.
- Avoid daytime napping.
- Identify the triggers of fatigue.
- Encourage the child/adolescent to plan meaningful goals, record activity achievement, and identify patterns of fatigue by using a notebook or diary.
- Link: Sleep for Youth. CHEO Sleep Hygiene handout
- Inform that fatigue can be worsened by low mood or stress.
- Inform that deconditioning can compound fatigue.
- Encourage a gradual return to school with accommodation (Domain 12: Return-to-School and Work).
11.3
Encourage patients with post-concussion fatigue to engage in cognitive activity and low-risk physical activity as soon as tolerated while staying below their symptom-exacerbation thresholds. Activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) should be resumed even if mild residual symptoms are present or whenever acute symptoms improve sufficiently to permit activity.
Level of Evidence: ![]() Gradual return to physical activity.
Gradual return to physical activity. ![]() Gradual return to cognitive activity.
Gradual return to cognitive activity.
See Recommendation 2.3.
- Refer select patients (e.g., highly-active or competitive athletes, those who are not tolerating a graduated return to physical activity, or those who are slow to recover) following acute injury to a medically supervised interdisciplinary team with the ability to individually assess sub-symptom threshold aerobic exercise tolerance and to prescribe aerobic exercise treatment. This exercise tolerance assessment can be as early as 48 hours following acute injury. Level of Evidence:
- Patients who are active may benefit from referral to a medically supervised interdisciplinary team with the ability to individually assess sub-symptom threshold aerobic exercise tolerance and to prescribe aerobic exercise treatment. This exercise tolerance assessment can be as early as 48 hours following acute injury. Level of Evidence:
Tool 2.6: Post-Concussion Information Sheet for examples of low-risk activities.
11.4
Consider referral to an interdisciplinary concussion team for patients with prolonged post-concussion fatigue (more than 4 weeks following the acute injury) to learn pacing techniques.
Level of Evidence: ![]()
11.5
Recommend a medical follow-up to re-assess clinical status if fatigue symptoms persist. Recommend an immediate medical follow-up in the presence of any deterioration. Consider early referral (before 4 weeks) to an interdisciplinary concussion team in the presence of modifiers that may delay recovery.
Level of Evidence: ![]() Medical follow-up.
Medical follow-up. ![]() Early referral in the presence of modifiers that may delay recovery.
Early referral in the presence of modifiers that may delay recovery.
Specialized interdisciplinary concussion care is ideally initiated for patients at elevated risk for a delayed recovery within the first two weeks post-injury.
Level of Evidence: ![]()
See Recommendation 2.1b: Note any modifiers that may delay recovery and use a clinical risk score to predict risk of prolonged symptoms.
Tools and Resources
References
Research papers that support the present guideline recommendations:
Botchway, E. N., Godfrey, C., Anderson, V., & Catroppa, C. (2019). A Systematic Review of Sleep-Wake Disturbances in Childhood Traumatic Brain Injury: Relationship with Fatigue, Depression, and Quality of Life. The Journal of Head Trauma Rehabilitation, 34(4), 241–256. https://doi.org/10.1097/HTR.0000000000000446
Bramley, H., Henson, A., Lewis, M. M., Kong, L., Stetter, C., & Silvis, M. (2017). Sleep Disturbance Following Concussion Is a Risk Factor for a Prolonged Recovery. Clinical Pediatrics, 56(14), 1280–1285. https://doi.org/10.1177/0009922816681603
Brooks, B. L., Sayers, P. Q., Virani, S., Rajaram, A. A., & Tomfohr-Madsen, L. (2019). Insomnia in adolescents with slow recovery from concussion. Journal of Neurotrauma, 36(16), 2391–2399. https://doi.org/10.1089/neu.2018.6257
Crichton, A., Oakley, E., Babl, F. E., Greenham, M., Hearps, S., Delzoppo, C., … Anderson, V. (2018). Predicting Fatigue 12 Months after Child Traumatic Brain Injury: Child Factors and Postinjury Symptoms. Journal of the International Neuropsychological Society, 24(3), 224–236. https://doi.org/10.1017/S1355617717000893
Howell, D. R., Oldham, J. R., Brilliant, A. N., & Meehan, W. P. (2019). Trouble Falling Asleep After Concussion Is Associated With Higher Symptom Burden Among Children and Adolescents. Journal of Child Neurology, 34(5), 256–261. https://doi.org/10.1177/0883073818824000
Kostyun, R. O., Milewski, M. D., & Hafeez, I. (2015). Sleep disturbance and neurocognitive function during the recovery from a sport-related concussion in adolescents. American Journal of Sports Medicine, 43(3), 633–640. https://doi.org/10.1177/0363546514560727
Landry-Roy, C., Bernier, A., Gravel, J., & Beauchamp, M. H. (2018). Executive Functions and Their Relation to Sleep Following Mild Traumatic Brain Injury in Preschoolers. Journal of the International Neuropsychological Society, 24(8), 769–780. https://doi.org/10.1017/S1355617718000401
Murdaugh, D. L., Ono, K. E., Reisner, A., & Burns, T. G. (2018). Assessment of Sleep Quantity and Sleep Disturbances During Recovery From Sports-Related Concussion in Youth Athletes. Archives of Physical Medicine and Rehabilitation, 99(5), 960–966. https://doi.org/10.1016/j.apmr.2018.01.005
Tham, S. W., Fales, J., & Palermo, T. M. (2015). Subjective and Objective Assessment of Sleep in Adolescents with Mild Traumatic Brain Injury. Journal of Neurotrauma, 32(11), 847–852. https://doi.org/10.1089/neu.2014.3559
Theadom, A., Starkey, N., Jones, K., Cropley, M., Parmar, P., Barker-Collo, S., & Feigin, V. L. (2016). Sleep difficulties and their impact on recovery following mild traumatic brain injury in children. Brain Injury, 30(10), 1243–1248. https://doi.org/10.1080/02699052.2016.1183171
Wiseman-Hakes, C., Gosselin, N., Sharma, B., Langer, L., & Gagnon, I. (2019). A Longitudinal Investigation of Sleep and Daytime Wakefulness in Children and Youth With Concussion. ASN Neuro, 11. https://doi.org/10.1177/1759091418822405
Research papers not associated with a current recommendation:
van Markus-Doornbosch, F., Peeters, E., van der Pas, S., Vlieland, T. V., & Meesters, J. (2019). Physical activity after mild traumatic brain injury: What are the relationships with fatigue and sleep quality? European Journal of Paediatric Neurology, 23(1), 53–60. https://doi.org/10.1016/j.ejpn.2018.11.002
Last update: November 16, 2019
 Domain 12: Return-to-school and Work
Domain 12: Return-to-school and Work
Introduction:
Overview:
- The return-to-school process should be coordinated by the school’s concussion management team and/or a point person in the school using the post-concussion return to school protocol and medical advice from the student’s health team (e.g., guidance counsellor, principal/vice principal, teacher, etc.).
- A key to the initial management of concussion is a gradual return to the school environment and activities after the initial period of modified activities (24-48 hours) and as soon as cognitive activities can be tolerated.
- Children/adolescents should be provided fast-acting temporary accommodations to their workload and schedule. Accommodations can be modified as symptoms resolve and/or when children/adolescents are caught up on missed workload and learning.
- Manage the gradual to school/activity/sport on a case-by-case basis.
- Post-concussion return to school and activity protocols: Living Guideline Return to School and Activities Protocols
Identifying and managing new or pre-existing school difficulties will:
- Clarify the most appropriate treatment and management options and accommodations based on the child/adolescent’s characteristics
- Promotes cognitive recovery and successful reintegration at school or work
- Support/assist return-to-school, engagement in daily activities, return to social engagement, management and treatment of symptoms
Tools to consider:
- Tool 2.0: Living Guideline Return to School and Activities Protocols (SEPT 2023 VERSION)
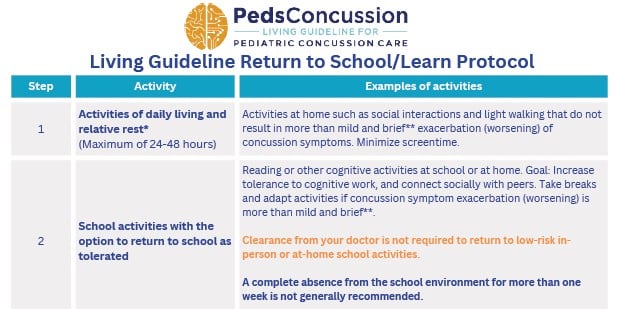
- Tool 1.2: Living Guideline Patient Information Sheet (SEPT 2023 VERSION)
- Tool 12.1: Concussion Implications and Interventions for the Classroom
- Tool 12.2: Template: Letter of Accommodation from the concussion care team to the school
- Tool 12.3: Template Letter of Accommodation from Physician to School
- Tool 12.4: Sample Letter/Email from School to Parents
- Link: CATT Return to School Strategy (2023 UPDATE COMING SOON)
- Link: CATT Student Return to Learn Plan (2023 UPDATE COMING SOON)
- Link: Heads Up Schools: Helping Students Recover from a Concussion: Classroom Tips for Teachers
- Link: Parachute’s Protocol for Return to Learn After a Concussion (Parachute Canada) (2023 UPDATE COMING SOON)
- Link: Post-Concussion Academic Accommodation Protocol (University of Oregon)
- Link: SCHOOLFirst: Enabling successful return to school for Canadian youth following a concussion (Holland Bloorview Kids Rehabilitation Hospital)
Recommendations
LEVEL OF EVIDENCE A = Consistent, good-quality, patient-oriented evidence (example: at least one large randomized control trial, meta-analysis or systematic review with homogeneity, or large, high- quality, multi-centre cohort study)B = Inconsistent or limited-quality patient-oriented evidence (example: smaller cohort studies, case studies or control trials with limitations)C = Consensus, usual practice, opinion or weaker-level evidence
12.1
This involves collaboration and communication among healthcare professionals, school-based professionals, the child/adolescent, and/or parents/caregivers.
Summary of tools to consider: These tools are suggestions for initiating a discussion to determine the best pathways for the student in learning environments.
- Tool 2.0: Living Guideline Return to School and Learn Protocol (UPDATED SEPT 2023)
- Tool 12.1: Concussion Implications and Interventions for the Classroom
- Tool 12.2: Template: Letter of Accommodation from the concussion care team to the school
- Tool 12.3: Template Letter of Accommodation from Physician to School
- Tool 12.4: Sample Letter/Email from School to Parents
- Link: CATT Return to School Strategy (UPDATE IN PROGRESS)
- Link: CATT Student Return to Learn Plan (UPDATE IN PROGRESS)
- Link: Heads Up Schools: Helping Students Recover from a Concussion: Classroom Tips for Teachers
- Link: Parachute’s Protocol for Return to Learn After a Concussion (Parachute Canada)
- Link: Post-Concussion Academic Accommodation Protocol (University of Oregon)
- Link: SCHOOLFirst: Enabling successful return to school for Canadian youth following a concussion (Holland Bloorview Kids Rehabilitation Hospital)
12.1a
Complete absence from the school environment for more than one week is not generally recommended. Children/adolescents should receive temporary academic accommodations (e.g, modifications to schedule, classroom environment and workload) to support a return to the school environment in some capacity as soon as possible.
Level of Evidence:![]()
- Tool 2.0: Living Guideline Return to School Protocol (UPDATED SEPT 2023)
- Tool 12.1: Concussion Implications and Interventions for the Classroom
- Tool 12.2: Template: Letter of Accommodation from the concussion care team to the school
- Tool 12.3: Template Letter of Accommodation from Physician to School
12.1b
Recommendation 2.3c: Recommend that patients avoid school activities associated with a risk of contact, fall, or collisions such as high speed and/or contact activities and full-contact sport that may increase the risk of sustaining another concussion during the recovery period. Advise/emphasize that returning to full-contact sport or high-risk activities before the child/adolescent has recovered increases the risk of delayed recovery and for sustaining another more severe concussion or more serious injury.
12.2
Assess for school difficulties using clinical judgment.
Level of Evidence: ![]()
Determine how much school the child/adolescent has missed post-concussion and how much missed workload the child/adolescent is expected to catch up on from missed school days.
Obtain school records to determine what issues may have been present prior to the concussion
School or cognitive difficulties may overlap with vision, vestibular, hearing, mental health, and social/family issues. Please assess.
- Domain 8: Mental Health
- Domain 9: Cognition
- Domain 10: Vision, Vestibular, and Oculomotor Function
12.3
Manage school difficulties.
Level of Evidence: ![]()
On re-evaluation, experienced health professionals (and school-based educational professionals where available) should manage school cognitive difficulties, provide accommodations, and reduce stressors. This should be done in collaboration with the child/adolescent, parents/caregivers, schools and/or employers to support success in the home, school, and community.
Refer to an interdisciplinary concussion team and/or a school-based educational professional (if available) if symptoms interfere with daily functioning more than 4 weeks following a concussion (Domain 9: Cognition). Refer for a formal evaluation if school difficulties may have been pre-existing.
Use tools to encourage reintegration within the school, employment, sports, social, and home environments.
Summary of tools to consider:
- Tool 2.0: Living Guideline Return to School Protocol (UPDATED SEPT 2023)
- Tool 12.1: Concussion Implications and Interventions for the Classroom
- Tool 12.2: Template: Letter of Accommodation from the Concussion Care Team to the School
- Tool 12.3: Template Letter of Accommodation from Physician to School
- Tool 12.4: Sample Letter/Email from School to Parents
- Link: SCHOOLFirst Handbook: Enabling successful return to school for Canadian youth following a concussion, page 6 (Holland Bloorview Kids Rehabilitation Hospital)
12.4
Encourage patients with school difficulties to engage in cognitive activity and low-risk physical activity as soon as tolerated. Activities that pose no/low risk of sustaining a concussion (no risk of contact, collision, or falling) should be resumed even if mild residual symptoms are present or whenever acute symptoms improve sufficiently to permit activity.
Level of Evidence: A Gradual return to physical activity. B Gradual return to cognitive activity.
See Recommendation 2.3.
12.5
Return-to-school and return-to-sport strategies can be performed simultaneously. Recommend that the child/adolescent return-to-school full-time at a full academic load, including writing exams without accommodations related to their concussion/post-concussion symptoms, before returning to full-contact sport or high-risk activities.
Level of Evidence: ![]()
See Domain 4: Medical clearance for full-contact sport or high-risk activity.
12.6
Prioritize return-to-school before return to work.
Level of Evidence: A Starting return to activity earlier.
For teens who work, please consult the “Guidelines for Concussion/ Mild Traumatic Brain Injury and Persistent Symptoms 3rd Edition For Adults (18+ years of age)” for recommendations on how to work with the adolescent’s employer regarding non-academic accommodations so that the adolescent can gradually return to work while promoting recovery.
Tools and Resources
Living Guideline Tools:
- Tool 12.1: Concussion Implications and Interventions for the Classroom
- Tool 12.2: Template: Letter of Accommodation from the Concussion Care Team to the School
- Tool 12.3: Template Letter of Accommodation from Physician to School
- Tool 12.4: Sample Letter/Email from School to Parents
Online Tools to Consider:
- CATT Return to School Strategy
- CATT Student Return to Learn Plan
- CATT Concussion Resources for School Professionals
- Heads Up Schools: Helping Students Recover from a Concussion: Classroom Tips for Teachers (CDC)
- Parachute’s Protocol for Return to Learn After a Concussion
- Post-Concussion Academic Accommodation Protocol (University of Oregon)
- SCHOOLFirst Handbook: Enabling successful return to school for Canadian youth following a concussion (Holland Bloorview Kids Rehabilitation Hospital)
References
To view and download the full citation list please use the interactive EPPImapper tool: https://pedsconcussion.com/evidence-map/
Updated list of citations included in the guideline (Sept 2023)
| Short title | Title | Year |
| Gomez (2023) | Stakeholder perspectives on navigating the pediatric concussion experience: Exploring the needs for improved communication across the care continuum | 2023 |
| Jo (2023) | Return-to-learn after sport-related concussion: does school level matter? | 2023 |
| Schmitz (2023) | Double Vision and Light Sensitivity Symptoms are Associated With Return-to-School Timing After Pediatric Concussion | 2023 |
| Shepherd (2023) | Unravelling the web: Experiences of adolescents returning to school following a concussion | 2023 |
| Vaughan (2023) | Association Between Early Return to School Following Acute Concussion and Symptom Burden at 2 Weeks Postinjury | 2023 |
| Berz (2022) | An intervention to improve knowledge and increase comfort of concussion management among school medical staff | 2022 |
| DeMatteo (2022) | School performance in youth after a concussion | 2022 |
| Kamba (2022) | Psychoeducational Interventions and Postconcussive Recovery in Children and Adolescents: A Rapid Systematic Review | 2022 |
| McAvoy (2022) | Return to Learn ECHO: Telementoring for School Personnel to Help Children Return to School and Learning After Mild Traumatic Brain Injury | 2022 |
| Mylabathula (2022) | Development of a concussion public policy on prevention, management and education for schools using expert consensus | 2022 |
| O’Brien (2022) | The School-Based Speech-Language Pathologist and Students With Concussion: An Examination of Evolving Knowledge and Confidence | 2022 |
| Takagi-Stewart (2022) | Physician recommended school accommodations and student outcomes following a mild traumatic brain injury among youth with persistent post-concussive symptoms | 2022 |
| Tang (2022) | Use of acute cognitive symptom cluster to predict return-to-learn duration following a sport-related concussion | 2022 |
| Jones (2021) | Parent and Teacher-Reported Child Outcomes Seven Years After Mild Traumatic Brain Injury: A Nested Case Control Study | 2021 |
| Keenan (2021) | Trajectories of Children’s Executive Function After Traumatic Brain Injury | 2021 |
| Yang (2021) | Association of Self-Paced Physical and Cognitive Activities Across the First Week Postconcussion With Symptom Resolution in Youth | 2021 |
| Conrick (2020) | Community-Engaged Approach to the Development and Implementation of a Student-Centered Return to Learn Care Plan After Concussion | 2020 |
| Dematteo (2020) | Effectiveness of return to activity and return to school protocols for children postconcussion: A systematic review | 2020 |
| DePadilla (2020) | Characteristics of Schools with Youth Sports Concussion-Related Educational Policies and Practices | 2020 |
| Holmes (2020) | Return to Learn: Academic Effects of Concussion in High School and College Student-Athletes | 2020 |
| Master (2020) | Characteristics of Concussion in Elementary School-Aged Children: Implications for Clinical Management | 2020 |
| Saleem (2020) | Sleep Symptoms Predict School Attendance After Pediatric Concussion | 2020 |
| Tsushima (2020) | Effects of a Single Concussion During the School Year on the Academic Performance and Neuropsychological Functioning of High School Athletes | 2020 |
| van Ierssel (2020) | Symptom Burden, School Function, and Physical Activity One Year Following Pediatric Concussion | 2020 |
| DeMatteo (2019) | Evaluating Adherence to Return to School and Activity Protocols in Children After Concussion | 2019 |
| DeMatteo (2019) | What Comes First: Return to School or Return to Activity for Youth After Concussion? Maybe We Don’t Have to Choose | 2019 |
| Gornall (2019) | Behavioral and Emotional Difficulties after Pediatric Concussion | 2019 |
| Lowry (2019) | Concussion and Academic Impairment Among U.S. High School Students | 2019 |
| Purcell (2019) | What factors must be considered in ‘return to school’ following concussion and what strategies or accommodations should be followed? A systematic review | 2019 |
| Russell (2019) | Academic outcomes following adolescent sport-related concussion or fracture injury: A prospective cohort study | 2019 |
| Sarmiento (2019) | From the CDC: A qualitative study of middle and high school professionals’ experiences and views on concussion: Identifying opportunities to support the return to school process | 2019 |
| Shendell (2019) | Developing and Piloting a School-Based Online Adolescent Student-Athlete Concussion Surveillance System | 2019 |
| Weber (2019) | School Nurses’ Management and Collaborative Practices for Student-Athletes Following Sport-Related Concussion | 2019 |
| Donnell (2018) | Concussion attitudes, behaviors, and education among youth ages 12–17: Results from the 2014 YouthStyles survey | 2018 |
| Green (2018) | Changes in working memory performance in youth following concussion | 2018 |
| Abbassi (2017) | Recovery progression and symptom resolution in sport-related mild traumatic brain injury | 2017 |
| Babcock (2017) | Adolescents with Mild Traumatic Brain Injury Get SMART: An Analysis of a Novel Web-Based Intervention | 2017 |
| Bellerose (2017) | Long-term brain-injury-specific effects following preschool mild TBI: A study of theory of mind. | 2017 |
| Rozbacher (2017) | The Effect of Concussion or Mild Traumatic Brain Injury on School Grades, National Examination Scores, and School Attendance: A Systematic Review | 2017 |
| Sufrinko (2017) | The Effectiveness of Prescribed Rest Depends on Initial Presentation After Concussion | 2017 |
| Swanson (2017) | Academic Difficulty and Vision Symptoms in Children with Concussion | 2017 |
| Ransom (2016) | Applying an Evidence-Based Assessment Model to Identify Students at Risk for Perceived Academic Problems following Concussion | 2016 |
| Russell (2016) | Academic Outcomes in High-School Students after a Concussion: A Retrospective Population-Based Analysis | 2016 |
| Wasserman (2016) | Academic Dysfunction After a Concussion Among US High School and College Students | 2016 |
| Baker (2015) | Factors Associated with Problems for Adolescents Returning to the Classroom after Sport-Related Concussion | 2015 |
| Iverson (2015) | Factors associated with concussion-like symptom reporting in high school athletes | 2015 |
| MacDonald (2015) | Reliability of a Computerized Neurocognitive Test in Baseline Concussion Testing of High School Athletes | 2015 |
| Moser (2015) | Examining prescribed rest as treatment for adolescents who are slow to recover from concussion | 2015 |
| Ransom (2015) | Academic Effects of Concussion in Children and Adolescents | 2015 |
| Ryan (2015) | Predictors of longitudinal outcome and recovery of pragmatic language and its relation to externalizing behaviour after pediatric traumatic brain injury | 2015 |
| Thomas (2015) | Benefits of Strict Rest After Acute Concussion: A Randomized Controlled Trial | 2015 |
| Van Beek (2015) | Mathematical Difficulties and White Matter Abnormalities in Subacute Pediatric Mild Traumatic Brain Injury | 2015 |
| Van Beek (2015) | Longitudinal changes in mathematical abilities and white matter following paediatric mild traumatic brain injury | 2015 |
| Brown (2014) | Effect of Cognitive Activity Level on Duration of Post-Concussion Symptoms | 2014 |
| Corwin (2014) | Characteristics of Prolonged Concussion Recovery in a Pediatric Subspecialty Referral Population | 2014 |
| Crowe (2014) | Verbal Ability and Language Outcome Following Traumatic Brain Injury in Early Childhood | 2014 |
| Darling (2014) | Evaluation of the Zurich Guidelines and Exercise Testing for Return to Play in Adolescents Following Concussion | 2014 |
| Gabbe (2014) | The association between hospitalisation for childhood head injury and academic performance: evidence from a population e-cohort study | 2014 |
| Gibson (2013) | The effect of recommending cognitive rest on recovery from sport-related concussion | 2013 |
| HOWELL (2013) | Effects of Concussion on Attention and Executive Function in Adolescents | 2013 |
Section A:
Concussion Recognition, Initial Medical Assessment, Management
Section C:
Biomarkers